Open Access Professional Publication
Author: Dr Samer Al-Diri
Author ORCID iD: 0009-0004-1908-0714 | https://orcid.org/0009-0004-1908-0714
Licence: Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Al-Diri S. Building Resilient Health Systems: A Healthcare Management Framework for Governance, Workforce Readiness and Digital Transformation. DrSamerAlDiri.com. Published 30 June 2026. Available at: https://drsameraldiri.com/building-resilient-health-systems-healthcare-management-framework/. Accessed 30 June 2026.
Executive Summary
Health systems today operate under conditions that were once considered exceptional. Workforce shortages, chronic disease burdens, climate disruption, fiscal constraint, technological complexity, fragile supply chains, migration, population ageing, and rising public expectations now form the normal operating environment. Resilience must therefore move beyond emergency planning and crisis slogans. It must become a core healthcare management capability [1,2].
This article is written for healthcare managers, hospital leaders, public health planners, ministry teams, humanitarian health actors, and digital transformation leaders who are responsible for maintaining essential services in resource-constrained, fragile, or rapidly changing environments.
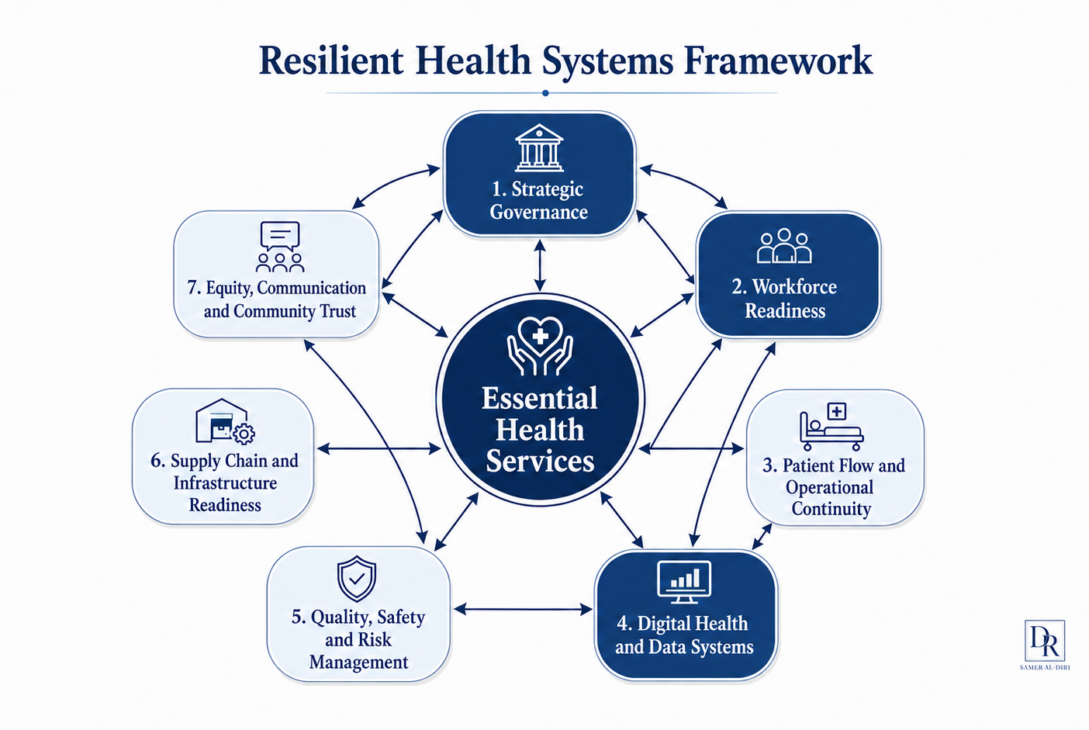
The article argues that resilient health systems are built through deliberate management capacity across seven integrated domains: strategic governance; workforce readiness; patient flow and operational continuity; digital health and data systems; quality, safety and risk management; supply chain and infrastructure readiness; and equity, communication and community trust. At the centre of these domains are essential health services: the practical promise a health system makes to its population and the clearest test of healthcare management when conditions deteriorate [3-7].
The Resilient Health Systems Management Framework, developed by Dr Samer Al-Diri, translates resilience from policy language into operational practice. It asks leaders to identify which services must continue, which failure points would cause harm first, which workforce and supply-chain risks require urgent action, which data are missing or unused, and which communities are most likely to lose access when capacity is constrained [8-11].
This revised article strengthens the framework in several ways. It adds methodological transparency, acknowledges legitimate critiques of resilience discourse, clarifies the evidence base, expands the four domains previously compressed, and includes a practical framework-application example.
It retains the original strategic emphasis on three high-leverage pillars: governance, workforce readiness, and digital transformation. These pillars receive deeper treatment because they connect the remaining domains and determine whether essential services can be protected in practice.
The framework is supported by a 100-day, 1-year, and 5-year roadmap. In the first 100 days, leaders should diagnose and stabilise. In the first year, they should build repeatable management systems. Over five years, they should institutionalise resilience so that it survives leadership transitions, funding cycles, and the pressures that will inevitably return.
The central message is direct: a resilient health system is one that can protect safe, essential, and equitable care when normal conditions deteriorate. The future healthcare manager is therefore not simply an administrator of routine processes. The future healthcare manager is a system steward responsible for connecting governance, workforce, operations, digital systems, quality, supply chains, and public trust around the continuity of essential care.
At a Glance
- Health system resilience is the management capability to protect safe, essential, and equitable care during disruption, uncertainty, or prolonged stress.
- Essential health services are the services that must continue because their failure rapidly harms patients, families, communities, and public trust.
- The Seven-Domain Resilient Health Systems Management Framework connects governance, workforce readiness, patient flow, digital systems, quality and safety, supply chains, and equity/community trust.
- Strategic governance, workforce readiness, and digital transformation are treated as high-leverage pillars because they coordinate, enable, and connect the other domains.
- Resilience must not be used to excuse chronic underfunding, shift responsibility to exhausted staff, or celebrate communities for coping with avoidable system weakness.
- A practical resilience roadmap should begin with service-protection diagnosis, then build management systems, then institutionalise resilience across leadership, financing, workforce, data, quality, procurement, and public communication.
How to use This Article
This article is designed to be read as a whole, but different readers may have different priorities. The guide below suggests where to begin based on role and interest.
For healthcare executives and decision-makers: start with the Executive Summary, the Seven-Domain Framework, and the 100-Day, 1-Year, and 5-Year Strategic Roadmap.
For healthcare managers, hospital leaders, and operational teams: focus on the Essential Services section, the Seven-Domain Framework, the three pillar sections on governance, workforce, and digital transformation, the Applying the Framework section, and the roadmap.
For public health planners, ministry teams, and humanitarian health actors: focus on the sections on essential services, methodology, resilience critique, strategic governance, workforce readiness, and the five-year institutional resilience horizon within the roadmap.
For digital health and AI leaders: focus on the Seven-Domain Framework, Digital Transformation Beyond Technology Theatre, the integration section, and the governance requirements for data protection, interoperability, cybersecurity, and human accountability.
For readers assessing professional expertise: the framework, methodology, critique engagement, integration logic, and conclusion represent the author’s approach to resilient healthcare management in its most concentrated form.
Contents
4. Introduction – The Healthcare Manager as System Architect
5. Methodology and Scope – How the Framework Was Developed
6. Essential Services as the True Test of Healthcare Management
7. The Resilient Health Systems Management Framework
8. What Makes Health System Governance Resilient? Strategic Governance for Adaptive Systems
9. Why Workforce Readiness Is Human Infrastructure
10. Why Digital Transformation Must Move Beyond Technology Theatre
11. Integration – How Governance, Workforce and Digital Systems Protect Essential Services
12. Applying the Framework – A Practical District Health Example
13. The 100-Day, 1-Year, and 5-Year Strategic Roadmap
14. Limitations and Appropriate Use of the Framework
15. Frequently Asked Questions
16. Conclusion – The Resilient Healthcare Leader
17. Author Bio, Suggested Citation, Licensing, Disclaimer, and References
Introduction – The Healthcare Manager as System Architect
A district health manager responsible for a small hospital and several rural clinics receives three reports within one hour. The central warehouse has lost cold-chain capacity. Two operating theatres are down because of staff absence. A flood warning has been issued for the catchment area. The manager must decide within the next sixty minutes which essential services will continue, which staff will be redeployed, which supplies must be safeguarded first, which referrals should be redirected, and how to communicate with the community. There is no time to wait for perfect information. There is only the system as it exists today.
This is where healthcare management becomes visible. It is the discipline that determines whether a health system can protect people when normal conditions deteriorate.
Healthcare management has often been treated as a supporting function: arranging staff, monitoring budgets, maintaining schedules, producing reports, coordinating procurement, and implementing decisions made elsewhere. These functions remain important, but they no longer describe the full responsibility of healthcare leadership. In modern health systems, the manager is a system architect: someone who designs the conditions under which safe, essential, and equitable care can continue during stress.
This shift matters because the pressures facing health systems are no longer rare or temporary. Workforce shortages, chronic disease burden, climate disruption, fiscal constraint, technological complexity, fragile supply chains, migration, population ageing, and rising public expectations now sit inside the ordinary operating environment [1,2,6,7]. Many systems are asked to deliver more care with fewer resources, more complexity, and less margin for error. In resource-constrained, fragile, rural, island, and humanitarian settings, these pressures may be immediate and persistent [28-30].
Resilience is often discussed through preparedness, emergency response, or recovery. These remain necessary, but they are incomplete. A system may have emergency plans and still fail because decision rights are unclear, staff are exhausted, referral pathways are blocked, medicines are unavailable, data are ignored, digital tools are unusable, or communities do not trust service changes [5,12,25-28]. Resilience must therefore be understood as a management capability, not only as a crisis document.
That capability begins with a clear object of protection: essential health services. These are the services that must continue because their failure rapidly harms patients, families, and communities [4,5]. Essential services are a clinical, operational, ethical, and managerial test. If leaders do not know what must be protected first, they cannot manage resilience effectively.
This article presents the Resilient Health Systems Management Framework, a seven-domain model for healthcare leaders working in resource-constrained, fragile, or rapidly changing environments. The framework places essential services at the centre and organises resilience around seven management domains: strategic governance; workforce readiness; patient flow and operational continuity; digital health and data systems; quality, safety and risk management; supply chain and infrastructure readiness; and equity, communication and community trust [1-11].
The purpose of the framework is practical. It is designed to help leaders ask better questions, identify predictable failure points, and organise action before disruption becomes collapse. Which services must continue if demand rises tomorrow? Who has authority to make urgent decisions? Which workforce gaps would cause failure first? Which supplies would run out first if delivery was delayed? Which data are missing, delayed, or unused? Which communities are likely to lose access first? These are the questions that determine whether care continues under real conditions.
The article examines three high-leverage pillars of resilience in greater depth. Strategic governance provides direction, accountability, and fair decision-making under uncertainty. Workforce readiness recognises health workers as the living infrastructure of care delivery. Digital transformation strengthens resilience only when it is problem-led, usable, interoperable, secure, equitable, and governed. These pillars do not replace the other four domains; they connect and enable them.
Before presenting the framework, the next section describes how it was developed, what evidence base supports it, and how its limits should be understood.
Methodology and Scope
The Resilient Health Systems Management Framework is an author-synthesised healthcare management framework. It was developed through a structured narrative synthesis of global health system guidance, peer-reviewed health system resilience literature, quality and safety literature, digital health governance guidance, workforce planning evidence, supply-chain literature, ethical priority-setting literature, and professional health system management experience across higher-resource and resource-constrained settings.
The review prioritised sources from the World Health Organization, OECD, World Bank, The Lancet Global Health, BMJ Global Health, Social Science & Medicine, Health Policy and Planning, Disasters, and other established health policy and health systems sources. It also drew on evidence from fragile and conflict-affected settings, low- and middle-income countries, climate-health preparedness, essential service continuity during COVID-19, task sharing, digital health implementation, and public trust [1-34].
The framework is informed by the author’s clinical, public health, and healthcare management experience, including work in higher-resource systems and resource-constrained island settings. It has not been formally validated, but it is designed to reflect recurring management questions encountered when services must be protected with limited reserve capacity.
Some resilience literature frames health systems primarily as complex adaptive systems [8,9]. This article acknowledges that perspective, but deliberately adopts a management framing. The aim is not to replace complexity-science analysis; it is to translate resilience into decisions, accountabilities, routines, and service-protection actions that healthcare leaders can use in practice.
The seven domains were selected because they represent recurring management failure points in health systems under stress: unclear authority, workforce fragility, blocked patient pathways, weak data and digital systems, unsafe care processes, disrupted supplies or infrastructure, and loss of equity or trust. The domains were then organised around essential health services because service continuity is the practical test through which resilience becomes visible.
Governance, workforce readiness, and digital transformation receive deeper treatment because they act as connector pillars. Governance decides priorities and accountability, workforce readiness determines delivery capacity, and digital systems make risk visible and actionable. Quality, supply chain, patient flow, and equity are equally essential, but these three pillars often determine whether the other domains can be coordinated when conditions deteriorate.
This is not a systematic review, formal Delphi consensus process, or empirically validated measurement instrument. It is a practical framework intended to help healthcare leaders diagnose vulnerabilities, prioritise action, and communicate resilience as a management discipline. Its value depends on local adaptation, multidisciplinary review, community engagement, and future empirical testing in different health system contexts.
Essential Services as the True Test of Healthcare Management
“The true test of healthcare management is not how a system performs on its easiest day. It is how it protects essential services when pressure rises.”
A health system may appear functional when staffing is adequate, supplies are available, referrals move smoothly, and demand follows expected patterns. The more important question is whether the same system can continue delivering safe, timely, and equitable care when these conditions change.
Essential health services are defined here as the services that must continue because interruption would rapidly cause avoidable harm. They include emergency care, primary care, maternal and child health, vaccination, essential medicines, diagnostics, chronic disease continuity, referral pathways, basic surgery and safe procedures, mental health support, rehabilitation where feasible, and core public health functions [4,5,31].
Defining the essential service package is not a purely technical exercise. It requires clinical judgement about harm prevention, operational judgement about feasibility, and ethical judgement about fairness under constraint. It should involve frontline clinicians, operational managers, public health teams, community representatives, and where relevant humanitarian partners. People working at the point of care and people depending on services often understand where failure would cause the most damage.
Once the essential service package is clear, leaders can ask which workforce groups are required, which medicines and supplies are critical, which referral pathways must remain open, which digital information is needed, which risks require escalation, and which communities are most likely to lose access first. Without this definition, resilience planning becomes vague. Everything appears important, but nothing is protected systematically.
Essential services also reveal the difference between activity and function. A clinic may be open, but if essential medicines are unavailable, the service is not fully functional. A hospital may have an emergency department, but if triage is unsafe, referral pathways are blocked, or staff are exhausted, patients remain at risk. A digital dashboard may show the number of consultations completed, while missing the fact that insulin, oxygen, or antibiotics are about to run out. Activity is not the same as protected function.
This is especially important in resource-constrained, fragile, rural, island, or humanitarian settings, where there may be little reserve capacity. A single supply-chain interruption, staff absence, transport disruption, delayed procurement decision, utility failure, or communication breakdown can halt services that communities depend on daily [26,28-30]. In these environments, resilience cannot be designed around ideal conditions. It must be designed around predictable constraints.
Essential services create an ethical test for healthcare management. Disruption rarely affects all people equally. Older people, children, pregnant women, people with disabilities, patients with chronic disease, remote communities, migrants, refugees, and low-income groups may lose access earlier and regain access later. A resilient system must therefore ask who can still reach services, who is excluded, and whose needs are becoming invisible.
The management task is to make essential services visible, prioritised, protected, and reviewed. This requires governance that defines priorities, workforce planning that safeguards delivery, operational systems that maintain patient flow, digital tools that make risks visible, supply chains that anticipate interruption, quality systems that protect safety, and communication that sustains equity and public trust. This is why the seven-domain framework places essential services at its centre.
The Resilient Health Systems Management Framework
Building on this understanding of essential services, the Resilient Health Systems Management Framework translates service protection into seven management functions. Health system resilience is a management discipline: a system becomes resilient when its management structures can protect essential services during stress, adapt to changing risks, support the workforce, maintain public trust, and continue safe care when ordinary operating conditions are disrupted [1,8-10].
The Resilient Health Systems Management Framework is a seven-domain model for healthcare leaders who need to protect essential services under constraint, disruption, or rapid change. Its purpose is to translate resilience into management functions that can be assessed, strengthened, and acted upon.
At the centre of the framework are essential health services. The seven surrounding domains are: strategic governance; workforce readiness; patient flow and operational continuity; digital health and data systems; quality, safety and risk management; supply chain and infrastructure readiness; and equity, communication and community trust.
These domains reflect a practical logic. Governance sets priorities, accountability, and decision pathways. Workforce readiness converts strategy into clinical and operational action. Patient flow and operational continuity determine whether people can reach the right service at the right time. Digital health and data systems provide visibility, coordination, and learning. Quality, safety and risk management protect patients from preventable harm. Supply chains and infrastructure provide the physical means of care. Equity, communication and community trust ensure that vulnerable populations are not abandoned when capacity is constrained.
The framework builds on established global health system thinking, including WHO health system strengthening guidance, primary health care, health system resilience, quality of care, climate resilience, workforce planning, digital health governance, and resilience literature in fragile settings [1-11,15-34]. Fragile-setting evidence repeatedly highlights the importance of legitimacy, local adaptation, basic service delivery, financing arrangements, workforce capacity, and relationships between state, non-state, and community actors [29,30]. The framework reorganises these insights around a single operational question: what must healthcare managers be able to govern, protect, and sustain when normal conditions break down?
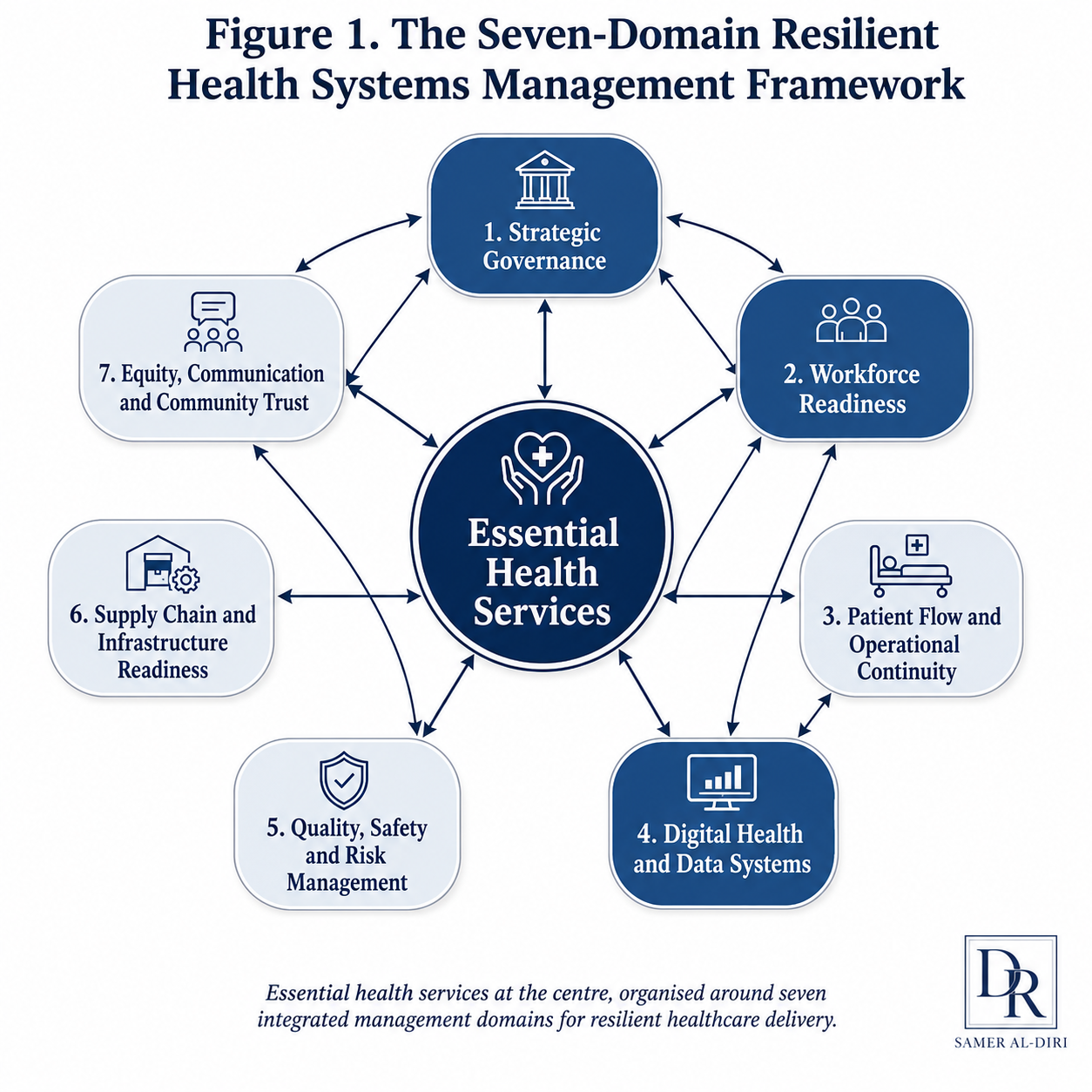
Figure 1. The Seven-Domain Resilient Health Systems Management Framework places essential health services at the centre and organises resilience around the management functions required to protect safe, accessible, and equitable care during disruption.
The Seven Domains
1. Strategic governance
Strategic governance is the first domain because resilience begins with decision-making. Without clear governance, disruption produces confusion. Leaders may not know who has authority, which services should be prioritised, how risks should be escalated, or how resources should be allocated. Strategic governance includes accountability, escalation pathways, intersectoral coordination, financing decisions, regulatory flexibility, anti-corruption safeguards, and fair priority-setting under uncertainty [12-14].
2. Workforce readiness
Workforce readiness is the second domain because health systems function through people. The workforce is the living infrastructure of healthcare delivery. It requires investment, maintenance, protection, supervision, and redundancy. Unlike physical infrastructure, the workforce can adapt, innovate, and make decisions under pressure, but only if it is supported, trained, protected, and trusted [15-18].
3. Patient flow and operational continuity
Patient flow and operational continuity determine whether services remain accessible in practice. A service may technically exist while patients are blocked by triage failure, transport disruption, referral delays, unsafe waiting areas, fragmented departments, weak scheduling, or unavailable diagnostics. Operational continuity requires managers to map how patients move through the system, identify bottlenecks, protect critical pathways, and redesign flow during stress.
In small island, rural, or conflict-affected contexts, a single broken referral pathway can convert a manageable condition into a preventable crisis. Managers therefore need continuity triggers: when to redirect referrals, which services should be decentralised temporarily, which clinics need outreach support, and how to communicate pathway changes to patients.
4. Digital health and data systems
Digital health and data systems provide visibility, coordination, and learning. However, digital tools strengthen resilience only when they solve real service problems and are integrated into workflows. Dashboards, electronic health records, AI-supported tools, supply-chain systems, telehealth, and predictive analytics can help leaders act earlier, but they can also increase fragmentation if they are poorly governed, poorly adopted, or disconnected from frontline practice [19-24,32-34].
5. Quality, safety and risk management
Quality, safety and risk management are essential because resilience must not mean keeping services open while care becomes unsafe. During disruption, medication errors, infection-control failures, delayed diagnosis, documentation gaps, communication breakdown, and unsafe improvisation may rise. Quality systems help leaders detect harm, learn from incidents, maintain standards, and protect patients when capacity is constrained [11,25].
Safety also requires practical realism. In a constrained setting, the safest plan is not always the most sophisticated plan; it is the plan that can be executed reliably. Simple escalation thresholds, visible safety huddles, stock-out alerts, referral tracking, infection-prevention routines, and structured incident review may protect patients more effectively than complex systems that no one can maintain.
6. Supply chain and infrastructure readiness
Supply chain and infrastructure readiness determine whether care can physically happen. Many health systems fail not because of lack of clinical knowledge, but because oxygen, medicines, diagnostics, equipment, utilities, transport, maintenance systems, or safe physical space become unavailable [26]. Resilience requires visibility over critical supplies, realistic procurement planning, maintenance capacity, backup systems, and infrastructure that can support essential services during stress [6,7].
Supply chains in resource-constrained settings are often affected by donor dependency, fragmented procurement, limited warehousing, delayed forecasting, transport vulnerability, single suppliers, customs delays, and weak maintenance arrangements. A resilient management approach therefore distinguishes between ordinary stock management and essential service protection. The question is not only what is in the store today, but which service will fail first if a critical item does not arrive.
7. Equity, communication and community trust
Equity, communication and community trust form the seventh domain because disruption is never socially neutral. Remote communities, older people, people with disabilities, migrants, refugees, low-income groups, and patients with chronic disease may lose access first and recover access last. Communication is therefore not a public-relations activity. It is a resilience function that supports appropriate service use, public cooperation, and legitimacy during difficult decisions [27,28].
Trust is especially important where service changes are unavoidable. If communities do not understand why a clinic timetable changed, why referrals were redirected, why elective procedures were postponed, or why outreach is prioritising certain groups, they may interpret operational decisions as neglect, favouritism, or abandonment. Transparent communication protects both service continuity and public legitimacy.
A Necessary Caution: Resilience Must Not Excuse Underinvestment
Resilience is valuable, but it can be misused. Critics of resilience discourse have warned that it may shift responsibility away from governments and institutions toward individuals, communities, and exhausted frontline staff; justify chronic underinvestment by celebrating the ability to cope; or become a technocratic substitute for political accountability [10]. These criticisms are legitimate. A management framework for resilience should not praise systems for surviving avoidable failure. It should expose where essential services are being protected only through staff sacrifice, informal workarounds, donor dependency, community burden, or unsafe improvisation.
For this reason, the framework treats resilience as an accountability discipline. It asks leaders to identify what must be funded, governed, staffed, supplied, communicated, measured, and protected. It makes visible who is carrying the cost of resilience and whether the system is adapting ethically or simply transferring burden to the least powerful. In this article, resilience means strengthening the conditions for safe and equitable service continuity. It does not mean normalising scarcity or accepting preventable system weakness.
How the Domains Work Together
The value of the framework is its integrative nature. Each domain matters individually, but none is sufficient alone. Governance without workforce capacity becomes policy without delivery. Workforce effort without data becomes activity without visibility. Digital systems without governance become unsafe or unused. Supply chains without accountability become hidden failure points. Quality systems without leadership become paperwork. Communication without trust becomes messaging without legitimacy.
For healthcare leaders, the framework serves three practical functions. First, it is a diagnostic tool: it allows a management team to assess which domains are weakest and where failure is most likely. Second, it is a planning architecture: it organises investment, workforce development, digital strategy, procurement, quality improvement, and public communication around a coherent structure. Third, it is a communication instrument: it helps leaders explain to boards, ministries, donors, staff, and communities why resilience requires integrated investment rather than isolated projects.
What Makes Health System Governance Resilient? Strategic Governance for Adaptive Systems
“A resilient health system is one that has the governance maturity to recognise disruption early, make decisions quickly, and protect essential services fairly.”
Resilience begins with governance because when disruption arrives, the quality of decision-making determines whether a system adapts or collapses. Health systems do not fail only because they lack beds, medicines, staff, or technology. They often fail because authority is unclear, priorities are contested, information is delayed, decisions are fragmented, and accountability is weak. Governance is the operating system through which a health system recognises risk, allocates resources, and protects essential services [12-14].
Strategic governance for resilience is different from routine administration. Routine administration manages established processes under expected conditions. Adaptive governance manages uncertainty, trade-offs, and incomplete information. It helps leaders decide which services must be protected, which risks must be escalated, which resources should be redirected, and which decisions cannot wait for ideal data.
When adaptive governance fails, the pattern is recognisable. Authority is contested, so no one decides. Priorities are unclear, so everything appears urgent and nothing is protected systematically. Information exists but is not trusted or acted upon. Coordination with other sectors is absent, so health services absorb the consequences of failures in transport, utilities, security, water, finance, or education. Financing is rigid, so managers cannot redirect resources when needs shift. Communities lose trust because they do not understand the rationale for difficult decisions.
The first requirement of adaptive governance is clarity of authority. Staff should know who can authorise service changes, redeploy personnel, approve emergency procurement, activate referral arrangements, communicate with the public, and request external support. During ordinary periods, unclear accountability may be hidden by informal workarounds. During disruption, it becomes dangerous.
The second requirement is prioritisation. No health system can protect everything equally during serious constraint. A resilient governance model defines which essential services must continue, which services may be modified temporarily, which groups require additional protection, and which thresholds trigger escalation. This does not mean rigid rationing. It means transparent, accountable priority-setting based on relevance, publicity, appeals, and enforcement principles associated with accountability for reasonableness [13,14].
The third requirement is decision-useful information. Governance does not require perfect digital maturity. Even a daily situation report with five indicators – service demand, workforce availability, critical supply levels, safety incidents, and community access concerns – can transform decision-making if the data are trusted, reviewed, and linked to accountability.
The fourth requirement is intersectoral coordination. Many threats to essential services begin outside the health sector: transport disruption, climate events, energy failure, food insecurity, conflict, migration, water and sanitation breakdown, school closure, financial instability, or supply-chain interruption [6,7,29,30]. Healthcare leaders need formal channels for coordination with local government, emergency services, finance, transport, utilities, community leaders, and humanitarian partners.
The fifth requirement is financing resilience. Preparedness is often underfunded because success can be invisible: when a crisis is prevented, no dramatic event proves the value of investment. Yet the absence of resilience financing creates predictable failure. Health systems need mechanisms for emergency procurement, stock protection, workforce surge, maintenance, referral continuity, digital backup, and rapid operational support [2,12].
The sixth requirement is regulatory agility. During disruption, rigid rules can delay necessary action, while uncontrolled improvisation can create safety risks. Adaptive governance sits between these extremes. It allows temporary, proportionate, documented, and accountable flexibility: modified staffing models, task-sharing arrangements, emergency procurement routes, referral adaptations, telehealth use, data-sharing protocols, or rapid credentialing.
The seventh requirement is integrity and trust. Governance systems must protect against corruption, favouritism, opaque procurement, selective service access, and politically driven decision-making. This is especially important where resources are scarce and public confidence is fragile. Anti-corruption safeguards, transparent procurement processes, documented decisions, and equity-focused monitoring are resilience tools [27,28].
Strategic governance must also protect the workforce. During stress, managers may focus on service outputs while underestimating what their decisions cost staff: exhaustion, moral distress, exposure to harm, and erosion of trust in leadership. A resilient governance model treats workforce protection as a core operational responsibility. It includes safe staffing thresholds, rest arrangements, psychological support, protection from violence or abuse, clear communication, and meaningful frontline involvement in operational decisions [15-18].
For boards, executives, and managers, the practical governance test is simple: can the system make timely, fair, and informed decisions when conditions deteriorate? If the answer is no, resilience will remain aspirational regardless of how many policies, committees, or digital tools exist.
Why Workforce Readiness Is Human Infrastructure
“The workforce is the living infrastructure through which resilience becomes real.”
If governance is the operating system of a resilient health system, the workforce is the human capacity through which care is delivered, adapted, and sustained. Buildings, equipment, medicines, and digital systems are essential. But none of them delivers care. Only people — trained, protected, supervised, and trusted — can do that. A health system can have written plans, modern facilities, and ambitious digital strategies yet still fail if the workforce is exhausted, poorly distributed, inadequately supported, or unable to adapt [15-18].
Workforce readiness is a core healthcare management responsibility. It asks whether the system has the right people, with the right skills, in the right places, supported by the right supervision, working under conditions that allow safe and sustained care. In constrained, fragile, or rapidly changing settings, this question becomes more important because there is often little spare capacity.
When workforce readiness fails, leaders lack visibility, so they do not know which services are vulnerable. Skill gaps remain hidden until a critical absence exposes them. Task sharing happens informally, without protocols or safeguards. Surge capacity is assumed rather than planned. Supervision is absent, leaving isolated staff to make decisions beyond their competence. Workforce protection is treated as secondary, so exhaustion, moral distress, and attrition accelerate.
The first element of workforce readiness is workforce visibility. Leaders cannot manage workforce risk if they do not know where staff are, what skills they have, which services depend on them, and where the most fragile points in the system are located. A resilient health system needs a practical workforce map: clinical roles, skill mix, rota vulnerabilities, single-person dependencies, supervision gaps, absenteeism patterns, training needs, and surge capacity.
The second element is skill-mix planning. Resilience depends not only on the number of workers, but on whether their skills match service needs. A hospital with staff on paper may still be unsafe if critical skills are concentrated in one person, one shift, or one department. Healthcare managers need to identify which competencies are essential for emergency care, maternal and child health, chronic disease continuity, infection prevention, diagnostics, pharmacy, referral coordination, and public health functions.
The third element is task sharing with safeguards. Task sharing can be safe and effective when it is planned, trained, supervised, monitored, and governed [17]. It becomes dangerous when it happens informally because no one else is available. Healthcare leaders should define which tasks can be shared, which tasks require escalation, what training is required, who supervises, how quality will be monitored, and how patients will be protected.
The fourth element is surge capacity. Health systems under stress need the ability to expand, redeploy, or reconfigure staffing without creating confusion about roles, accountability, or clinical safety. Surge capacity may include reserve rosters, cross-training, rapid orientation, flexible team structures, emergency credentialing, tele-support, temporary redeployment, and coordination with external partners. It cannot be invented during the emergency itself.
The fifth element is supervision and decision support. Workforce readiness is not achieved by placing staff in difficult situations and expecting them to solve problems alone. Staff need clinical guidance, escalation routes, peer support, and real-time problem-solving. This is particularly important when less experienced staff are redeployed, when task sharing is expanded, or when services are operating with reduced capacity.
The sixth element is workforce protection. A system cannot claim resilience while consuming its staff. During disruption, health workers may face fatigue, moral distress, violence, infection risk, family pressure, uncertainty, and public criticism. Workforce protection requires safe staffing thresholds, rest arrangements, psychological support, access to protective equipment, fair communication, protection from abuse, and visible leadership presence.
The seventh element is retention and professional trust. In fragile and resource-constrained systems, workforce loss can be more damaging than infrastructure loss because skills are difficult to replace quickly. Retention depends on pay and conditions, but also on fairness, professional respect, career development, supervision, safety, and involvement in decision-making.
Workforce readiness also requires equity within the workforce. Women, junior staff, migrant workers, community health workers, and lower-paid cadres often carry a large share of service delivery while having less influence over decisions. A resilient workforce strategy must recognise who is doing the work, who is exposed to risk, who has voice, and who is excluded from leadership pathways.
For healthcare leaders, the practical workforce question is not simply, “How many staff do we have?” The better question is: “Can this workforce maintain essential services safely when capacity is constrained?” That question shifts attention from headcount to capability, distribution, protection, supervision, and adaptability.
Why Digital Transformation Must Move Beyond Technology Theatre
“Digital transformation fails when technology is purchased before the problem, workflow, workforce, and governance model have been properly defined.”
Digital transformation is frequently promoted as the solution to healthcare resilience. In reality, it is a tool that strengthens resilience only when it is governed, usable, trusted, and connected to the daily work of care delivery. A health system does not become resilient because it purchases software, installs dashboards, or announces an artificial intelligence strategy. It becomes more resilient when digital systems help leaders see risks earlier, coordinate services better, support the workforce, protect patients, and maintain essential services during stress [19-24,32-34].
Technology theatre occurs when digital investment creates the appearance of modernisation without solving the operational problem. It may appear as a dashboard no one uses, an electronic record that increases documentation burden, an AI tool with unclear accountability, a telehealth service that excludes low-connectivity communities, or a data platform that cannot communicate with procurement, workforce, or referral systems. In each case, technology is present, but resilience is not strengthened.
The first requirement for resilient digital transformation is problem-led design. Leaders should begin with the operational failure they need to prevent: delayed referral, missed stock-out, unsafe triage, poor follow-up, workforce absence, lack of visibility, or weak community access. Only then should they decide which digital tool, if any, can help.
The second requirement is workflow integration. A digital system that does not fit the workflow will either be ignored or will create additional work. Frontline staff should be involved early, not invited to adopt a completed system after procurement. Usability, training, feedback, and adaptation are not secondary details. They determine whether the tool becomes part of care delivery.
The third requirement is interoperability. Resilience depends on connected information. If workforce data, patient flow data, supply-chain data, quality data, and community access information remain in separate systems, leaders cannot see how risks interact. Interoperability does not always require sophisticated infrastructure. It requires agreed data definitions, ownership, standards, and routines for using information in decisions [19,22,23].
The fourth requirement is governance and accountability. Digital health and AI systems influence clinical decisions, operational priorities, workforce allocation, public health surveillance, procurement, and access to care. They require human accountability, ethical governance, transparency, data protection, and review mechanisms [20,21]. No algorithm should become a hidden decision-maker in a health system without clear oversight.
The fifth requirement is cyber resilience and privacy protection. As health systems digitise, cyber risk becomes a patient safety and service continuity risk. A ransomware attack, data breach, system outage, or loss of network connectivity can disrupt appointments, prescriptions, laboratory results, imaging, theatre lists, procurement, and communication. Cybersecurity is therefore not a technical afterthought; it is part of essential service protection [22,24].
The sixth requirement is equity. Digital transformation can reduce distance, improve follow-up, and support remote care. It can also widen exclusion when patients lack devices, connectivity, language access, digital literacy, disability support, or trust. A resilient digital strategy asks who benefits, who is excluded, and what analogue or assisted pathways remain available.
The seventh requirement is learning. Digital systems should help teams learn from service disruptions, not merely report activity. A useful digital resilience dashboard should show where essential services are at risk: staffing gaps, medicine levels, referral delays, safety incidents, demand surges, equipment downtime, and access concerns. The dashboard is valuable only if someone is responsible for reviewing it and acting on it.
The practical digital question is therefore not, “What technology should we buy?” It is: “Which essential service risk must become visible, actionable, and accountable?” When digital transformation begins with that question, it can strengthen resilience. When it begins with procurement, it risks becoming technology theatre.
Integration – How Governance, Workforce and Digital Systems Protect Essential Services
Section 7 described how all seven domains interact. This section focuses specifically on how governance, workforce, and digital systems form the management loop that connects the entire framework.
The seven-domain framework becomes most useful when leaders understand how the domains interact. Resilience is rarely lost through one isolated weakness. It is usually lost through combinations: a decision delay that worsens a workforce shortage, a workforce shortage that blocks patient flow, a supply failure that is not visible in the data, a digital tool that lacks governance, a communication failure that damages trust, or a safety incident that no one learns from.
The three high-leverage pillars – governance, workforce, and digital systems – are emphasised because they connect the whole framework. Governance decides what matters and who is accountable. Workforce readiness determines whether action can be delivered. Digital systems determine whether leaders can see, coordinate, and learn. Together, they create the management loop through which essential services are protected.
The loop begins with service definition. Leaders identify the essential services that must continue. Governance then assigns authority and accountability. Workforce planning maps the people and competencies required. Digital systems make demand, capacity, supplies, referrals, and safety visible. Quality systems detect harm. Supply-chain systems protect the physical means of care. Equity and communication systems maintain legitimacy and access. The loop repeats as conditions change.
This integration is particularly important in resource-constrained settings. A small hospital may not have advanced digital infrastructure, large reserve staffing, or redundant supply systems. But it can still create a disciplined resilience loop: a weekly essential-service review, a workforce vulnerability map, a critical-supply tracker, a referral-risk list, a safety huddle, and a community communication plan. These are management behaviours, not luxury technologies.
Empirical literature on essential service continuity during COVID-19 reinforces this logic. Cross-country analyses in low- and middle-income countries identified context-specific essential service definitions, service adaptations, data availability, and equitable technology access as important factors in maintaining services, while also emphasising the need for further evaluation [33]. Studies from fragile and conflict-affected settings similarly show that resilience depends on governance, local adaptation, workforce arrangements, financing, legitimacy, and relationships, not on single interventions alone [29,30].
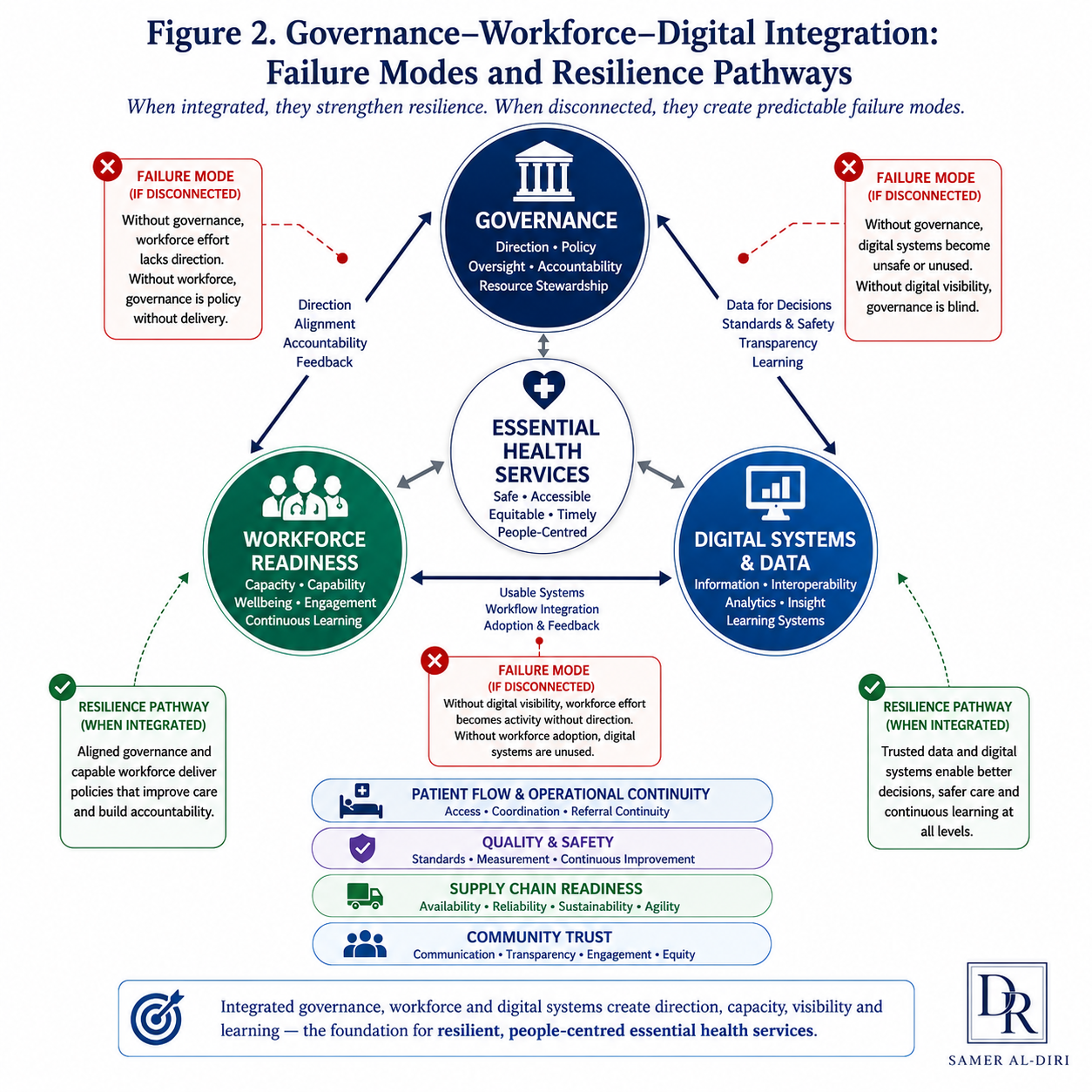
Figure 2. Governance, workforce readiness, and digital systems form an integrated management loop for protecting essential services. Governance defines priorities and accountability; workforce readiness enables delivery; digital systems provide visibility, coordination, and learning.
Applying the Framework – A Practical District Health Example
Consider a district health team responsible for one small hospital, six primary care clinics, two mobile outreach teams, and a population with high chronic disease burden. The district faces three immediate pressures: medicine deliveries have become unreliable, two senior nurses are leaving, and seasonal flooding may affect two remote communities.
Using the framework, the team begins with essential services. It defines the services that must continue during the next three months: emergency triage, maternal and child health, vaccination, diabetes and hypertension medicines, essential diagnostics, basic procedures, referrals for high-risk patients, and outreach for remote communities. This list becomes the operational protection package.
The team then tests each domain. Governance: who can authorise temporary service changes, emergency purchasing, and referral redirection? Workforce: which services depend on single individuals, which staff can be cross-trained, and who supervises task sharing? Patient flow: which clinics will become inaccessible if flooding occurs, and what alternative routes exist? Digital systems: what minimum daily information is needed on service demand, stock levels, staff availability, referrals, and safety incidents? Quality and safety: which standards cannot be compromised, even if services are modified? Supply chain: which medicines, diagnostics, and equipment items would cause service failure if absent? Equity and communication: which communities need advance information, transport support, or outreach adaptation?
The team then resolves three decisions rather than leaving them as open questions. First, the district director authorises a temporary service-change protocol: if flood access is lost or stock falls below seven days, the clinic lead may shift stable chronic-disease follow-up to outreach or tele-support, but emergency, maternal, child-health, and vaccination pathways remain protected. Second, the nursing lead creates a supervised task-sharing rota so two additional nurses can support diabetes and hypertension medicine continuity, with escalation rules for unstable patients. Third, the pharmacy officer identifies five critical items – insulin, antihypertensives, antibiotics, vaccines, and basic diagnostic consumables – and links each to minimum stock levels, supplier contact points, and transport contingencies.
The output is not a long plan that sits unread. It is a simple action board: red risks, named owners, deadlines, escalation triggers, and communication tasks. The district may decide to protect one cold-chain backup route, cross-train nurses for chronic disease follow-up, establish a weekly critical-stock call with suppliers, pre-position emergency medicines before flood season, create referral agreements with neighbouring facilities, and issue community messages explaining temporary service arrangements. The framework turns resilience from an abstract ambition into a sequence of management decisions.
The 100-Day, 1-Year, and 5-Year Strategic Roadmap
The framework should be implemented in stages. Trying to build comprehensive resilience in one step risks producing an unrealistic plan. Sequencing matters. The first 100 days should diagnose and stabilise. The first year should build repeatable management systems. The five-year horizon should institutionalise resilience so that it survives leadership transitions, funding cycles, and future shocks.
The roadmap below translates the framework into three practical horizons: immediate diagnosis and stabilisation, first-year system-building, and long-term institutional resilience. Each phase links strategic aim, executive priorities, and management output so that resilience becomes a sequence of leadership decisions rather than a general aspiration.
| Time horizon & strategic aim | Executive priorities | Management output |
| First 100 days Diagnose and stabilise | • Define the essential service package • Map governance, workforce, supply-chain, operational and digital vulnerabilities • Create a minimum leadership dashboard • Introduce immediate stabilisation measures | Clear baseline with visible risks, named owners and early protection of essential services |
| First year Build repeatable management systems | • Formalise governance pathways • Develop workforce readiness and task-sharing safeguards • Strengthen patient-flow, referral and supply monitoring • Improve digital/data governance, safety review and communication routines | Functional resilience capacity embedded into routine management |
| First five years Institutionalise resilience | • Embed resilience in financing, workforce strategy and procurement • Mature digital architecture, regulation and emergency preparedness • Develop leadership pipelines and public health planning • Institutionalise quality learning and community accountability | Sustainable health-system resilience that survives disruption, leadership change and shifting external pressures |
Figure 3. The 100-Day, 1-Year, and 5-Year Strategic Roadmap translates the Resilient Health Systems Management Framework into sequenced action: diagnose and stabilise, build management systems, and institutionalise resilience.
First 100 Days – Diagnose and Stabilise
In the first 100 days, leaders should not attempt to redesign the entire health system. They should identify which essential services are most vulnerable and stabilise the risks most likely to cause immediate harm. This means creating a practical essential-service list, mapping workforce dependencies, identifying critical supplies, reviewing referral pathways, establishing clear escalation rights, and agreeing on a small set of decision-useful indicators.
A 100-day diagnostic should be short enough to be used. It should answer: which essential services must continue; what would make them fail first; who owns each risk; what action is required now; what needs funding; what needs escalation; and which communities require additional protection. The output should be reviewed regularly by the leadership team, not stored as a static report.
First Year – Build Management Systems
In the first year, the task shifts from stabilisation to system-building. Leaders should convert the diagnostic into repeatable management routines. This includes scheduled resilience reviews, workforce development plans, stock and maintenance monitoring, referral continuity processes, quality and safety learning, digital governance, community communication protocols, and board or ministry reporting.
The first year is also the period for formalising task sharing, strengthening supervision, aligning financing with essential service protection, and building data routines that staff trust. The aim is not sophistication. The aim is reliability. A simple system used every week is more resilient than an advanced system used only during a crisis.
Five Years – Institutionalise Resilience
Over five years, resilience should become part of the institution rather than the personality of one leader. This requires embedding resilience into financing, procurement, workforce planning, quality systems, digital architecture, emergency preparedness, regulatory pathways, leadership development, and community accountability. It also requires measuring whether essential services remain accessible, safe, and equitable when conditions deteriorate.
Institutionalisation means that resilience survives turnover, political change, donor cycles, technology replacement, and repeated operational stress. The goal is not a perfect system. The goal is a system that learns, adapts, protects its workforce, and continues essential care with integrity.
Limitations and Appropriate Use of the Framework
This framework has several limitations. First, it is a management framework developed through narrative synthesis and professional interpretation. It has not yet been empirically validated as a measurement instrument. Second, it may require significant adaptation for different health system models, financing structures, governance arrangements, cultures, and regulatory settings. Third, it is written from a healthcare management and health system perspective, not as a full community-led participatory framework. Community engagement is essential for local application.
Fourth, the evidence base for health system resilience remains uneven. Many sources are normative guidance documents, conceptual frameworks, qualitative studies, or context-specific case studies. They provide strong direction, but not always causal proof that one sequence of interventions improves outcomes in all settings. Leaders should therefore treat the framework as a structured starting point for diagnosis, prioritisation, and local adaptation rather than as a universal formula.
Fifth, the framework should not be used to justify underinvestment. Where essential services fail because staff are too few, medicines are unavailable, infrastructure is unsafe, or communities are excluded, the solution is not to praise resilience. The solution is to correct the conditions that make unsafe coping necessary.
Frequently Asked Questions
What is health system resilience?
Health system resilience is the capability of a health system to anticipate, absorb, adapt to, recover from, and learn from disruption while protecting safe, essential, and equitable care. In this article, resilience is treated as a healthcare management capability, not only as emergency preparedness.
What are essential health services?
Essential health services are the services that must continue because their interruption rapidly harms patients, families, communities, and public trust. They include emergency care, primary care, maternal and child health, vaccination, essential medicines, diagnostics, chronic disease continuity, referral pathways, basic procedures, mental health support, and core public health functions.
What are the seven domains of the Resilient Health Systems Management Framework?
The seven domains are strategic governance; workforce readiness; patient flow and operational continuity; digital health and data systems; quality, safety and risk management; supply chain and infrastructure readiness; and equity, communication and community trust.
Why does the article emphasise governance, workforce readiness, and digital transformation?
These three pillars receive deeper treatment because they connect the framework. Governance defines priorities and accountability. Workforce readiness enables delivery. Digital systems provide visibility, coordination, and learning. Together, they determine whether the other domains can function during stress.
How should healthcare leaders begin applying the framework?
Leaders should begin with a simple essential-service diagnostic: identify which services must continue, what would cause them to fail first, who owns each risk, what data are needed, which supplies and workforce groups are critical, and which communities are most likely to lose access. The first objective is to diagnose and stabilise before attempting large-scale redesign.
What if an organisation lacks the resources to implement all seven domains at once?
The framework does not require leaders to fix everything simultaneously. Start with the essential services most likely to fail and the risks most likely to cause harm. In many settings, the first practical actions are modest: clarify decision rights, protect one critical supply chain, map workforce single points of failure, agree on referral triggers, and communicate service changes clearly. Resilience begins with disciplined prioritisation, not large-scale expenditure alone.
How can leaders justify resilience investment when there is no visible crisis?
Leaders can frame resilience investment as service continuity, patient safety, workforce protection, financial risk reduction, and public trust. The strongest argument is concrete: identify which essential service would fail first, what harm that failure would cause, and what low-cost action would reduce that risk before disruption occurs.
Conclusion – The Resilient Healthcare Leader
The future of healthcare management will belong to leaders who can connect governance decisions to frontline service delivery, technology to workflow, workforce protection to patient safety, supply-chain visibility to essential services, and public health goals to operational decisions. These leaders will not measure success only by activity, infrastructure, or digital sophistication. They will measure it by the continuity of safe, essential, and equitable care when communities need it most.
Resilience is demonstrated when patients still receive essential care, when staff remain protected and trusted, when leaders act before collapse, when communities understand difficult decisions, and when the system learns openly from what it has been through and changes as a result.
The resilient healthcare leader is not the person who promises that disruption will never happen. Disruption will happen. The resilient leader is the person who knows what must be protected, who must be involved, which risks are most dangerous, which decisions cannot wait, which data matter, which staff need protection, and which communities are most likely to be left behind.
Every healthcare leader reading this article can begin with one question: if pressure rises in my system tomorrow, which essential service would fail first – and what would it take to protect it starting today? That is the work of resilient healthcare management. That is the work of the resilient healthcare leader.
Author Bio
Dr Samer Al-Diri is a UK-trained ophthalmologist with specialist clinical training in retina and academic postgraduate training in ophthalmology and public health. He holds an MSc in Ophthalmology from University College London and an MPH with Merit from City, University of London. His work sits at the intersection of ophthalmology, public health, healthcare management, digital health, and resilient health system strengthening.
Dr Al-Diri has clinical, public health, and health system experience across the United Kingdom, the United Arab Emirates, and resource-constrained island settings. His professional interests include essential health services, healthcare governance, workforce readiness, digital transformation, and artificial intelligence in healthcare, with a focus on resource-constrained and fragile settings.
He translates clinical insight, public health thinking, and healthcare management experience into practical frameworks for safer, more equitable, and more resilient health systems.
Suggested Citation
Al-Diri S. ORCID: 0009-0004-1908-0714. Building Resilient Health Systems: A Healthcare Management Framework for Governance, Workforce Readiness and Digital Transformation. DrSamerAlDiri.com. Published 30 June 2026. Available at: https://drsameraldiri.com/building-resilient-health-systems-healthcare-management-framework/. Accessed 30 June 2026.
Open Access Licensing Statement
This article is published as an open-access professional and educational resource.
© Dr Samer Al-Diri. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Licence (CC BY-NC-ND 4.0).
You may share this work for non-commercial purposes with appropriate attribution, provided it is not modified, adapted, or used for commercial purposes without prior written permission.
Full licence terms: https://creativecommons.org/licenses/by-nc-nd/4.0/
Disclaimer
This article is provided for educational, professional, and informational purposes only. It does not constitute medical advice, legal advice, policy instruction, or a substitute for local clinical, regulatory, operational, or governance decision-making.
Health-system planning, digital health implementation, workforce strategy, emergency preparedness, and service-resilience decisions should be adapted to local context, available resources, regulatory requirements, patient needs, and professional guidance.
This article represents the author’s intellectual framework, professional interpretation, and responsibility for the final published content. The views expressed are those of the author and do not necessarily represent the views of any current or previous employer, institution, organisation, government body, or professional affiliation.
References
[1] World Health Organization. Building health systems resilience for universal health coverage and health security during the COVID-19 pandemic and beyond: WHO position paper. Geneva: World Health Organization; 2021. Available at: https://www.who.int/publications/i/item/WHO-UHL-PHC-SP-2021.01
[2] OECD. Ready for the Next Crisis? Investing in Health System Resilience. OECD Health Policy Studies. Paris: OECD Publishing; 2023. Available at: https://doi.org/10.1787/1e53cf80-en
[3] World Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action. Geneva: World Health Organization; 2007. Available at: https://www.who.int/publications/i/item/everybody-s-business—-strengthening-health-systems-to-improve-health-outcomes
[4] World Health Organization and United Nations Children’s Fund. Operational Framework for Primary Health Care: Transforming Vision into Action. Geneva: World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/9789240017832
[5] World Health Organization. Maintaining Essential Health Services: Operational Guidance for the COVID-19 Context. Interim guidance, 1 June 2020. Geneva: World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-essential_health_services-2020.2
[6] World Health Organization. Operational Framework for Building Climate Resilient and Low Carbon Health Systems. Geneva: World Health Organization; 2023. Available at: https://www.who.int/publications/i/item/9789240081888
[7] World Health Organization. WHO Guidance for Climate-Resilient and Environmentally Sustainable Health Care Facilities. Geneva: World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/9789240012226
[8] Blanchet K, Nam SL, Ramalingam B, Pozo-Martin F. Governance and capacity to manage resilience of health systems: towards a new conceptual framework. International Journal of Health Policy and Management. 2017;6(8):431-435. doi:10.15171/ijhpm.2017.36
[9] Biddle L, Wahedi K, Bozorgmehr K. Health system resilience: a literature review of empirical research. Health Policy and Planning. 2020;35(8):1084-1109. doi:10.1093/heapol/czaa032
[10] Witter S, Thomas S, Topp SM, Barasa E, Chopra M. Health system resilience: a critical review and reconceptualisation. The Lancet Global Health. 2023;11(9):e1454-e1458. doi:10.1016/S2214-109X(23)00279-6
[11] Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet Global Health. 2018;6(11):e1196-e1252. doi:10.1016/S2214-109X(18)30386-3
[12] World Bank Group. High-Performance Health Financing for Universal Health Coverage: Driving Sustainable, Inclusive Growth in the 21st Century. Washington, DC: World Bank; 2019. Available at: https://www.worldbank.org/en/topic/universalhealthcoverage/publication/high-performance-health-financing-for-universal-health-coverage-driving-sustainable-inclusive-growth-in-the-21st-century
[13] Daniels N. Accountability for reasonableness: establishing a fair process for priority setting is easier than agreeing on principles. BMJ. 2000;321(7272):1300-1301. doi:10.1136/bmj.321.7272.1300
[14] Byskov J, Marchal B, Maluka S, et al. The accountability for reasonableness approach to guide priority setting in health systems within limited resources: findings from action research at district level in Kenya, Tanzania, and Zambia. Health Research Policy and Systems. 2014;12:49. doi:10.1186/1478-4505-12-49
[15] World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals. Human Resources for Health Observer Series No. 17. Geneva: World Health Organization; 2016. Available at: https://www.who.int/publications/i/item/9789241511407
[16] World Health Organization. Working for Health 2022-2030 Action Plan. Geneva: World Health Organization; 2022. Available at: https://www.who.int/publications/i/item/9789240063341
[17] World Health Organization. Optimizing Health Worker Roles to Improve Access to Key Maternal and Newborn Health Interventions Through Task Shifting. Geneva: World Health Organization; 2012. Available at: https://www.who.int/publications/i/item/9789241504843
[18] Cometto G, Buchan J, Dussault G. Developing the health workforce for universal health coverage. Bulletin of the World Health Organization. 2020;98(2):109-116. doi:10.2471/BLT.19.234138
[19] World Health Organization. Global Strategy on Digital Health 2020-2025. Geneva: World Health Organization; 2021. Available at: https://www.who.int/publications/i/item/9789240020924
[20] World Health Organization. Ethics and Governance of Artificial Intelligence for Health: WHO Guidance. Geneva: World Health Organization; 2021. Available at: https://www.who.int/publications/i/item/9789240029200
[21] World Health Organization. Ethics and Governance of Artificial Intelligence for Health: Guidance on Large Multi-Modal Models. Geneva: World Health Organization; 2025. Available at: https://www.who.int/publications/i/item/9789240084759
[22] OECD. Health Data Governance for the Digital Age: Implementing the OECD Recommendation on Health Data Governance. Paris: OECD Publishing; 2022. Available at: https://www.oecd.org/en/publications/health-data-governance-for-the-digital-age_68b60796-en.html
[23] Digital Public Goods Alliance. Digital Public Goods Standard. Available at: https://www.digitalpublicgoods.net/standard.Accessed 26 June 2026.
[24] World Health Organization Regional Office for Europe. Cybersecurity and Privacy Maturity Assessment and Strengthening for Digital Health Information Systems. Copenhagen: WHO Regional Office for Europe; 2025. Available at: https://www.who.int/europe/publications/i/item/WHO-EURO-2025-11827-51599-78854
[25] World Health Organization. Quality Health Services: A Planning Guide. Geneva: World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/9789240011632
[26] Yadav P. Health product supply chains in developing countries: diagnosis of the root causes of underperformance and an agenda for reform. Health Systems & Reform. 2015;1(2):142-154. doi:10.4161/23288604.2014.968005
[27] World Health Organization. Communicating Risk in Public Health Emergencies: A WHO Guideline for Emergency Risk Communication Policy and Practice. Geneva: World Health Organization; 2017. Available at: https://iris.who.int/handle/10665/259807
[28] Gilson L. Trust and the development of health care as a social institution. Social Science & Medicine. 2003;56(7):1453-1468. doi:10.1016/S0277-9536(02)00142-9
[29] Newbrander W, Waldman R, Shepherd-Banigan M. Rebuilding and strengthening health systems and providing basic health services in fragile states. Disasters. 2011;35(4):639-660. doi:10.1111/j.1467-7717.2011.01235.x
[30] Truppa C, Gaillard JC, Barasa E, et al. Health systems resilience in fragile and conflict-affected settings: a systematic scoping review. Conflict and Health. 2024;18:2. doi:10.1186/s13031-023-00553-2
[31] World Health Organization and United Nations Children’s Fund. Primary Health Care Measurement Framework and Indicators: Monitoring Health Systems Through a Primary Health Care Lens. Geneva: World Health Organization and UNICEF; 2022. Available at: https://www.who.int/publications/i/item/9789240044210
[32] Yi S, Yam ELY, Cheruvettolil K, Linos E, Gupta A, Palaniappan L, Rajeshuni N, Vaska KG, Schulman K, Eggleston KN. Perspectives of Digital Health Innovations in Low- and Middle-Income Health Care Systems From South and Southeast Asia. Journal of Medical Internet Research. 2024;26:e57612. doi:10.2196/57612
[33] Guha M, Cohen Tanugi-Carresse A, Mullen L, Bennett S, Wanyenze RK, Prado AM, et al. Maintaining essential health services during COVID-19: cross-country lessons of health system resilience from Asia, Sub-Saharan Africa and Latin America. BMJ Global Health. 2025;8(Suppl 6):e013392. doi:10.1136/bmjgh-2023-013392
[34] Dugani B, Juma P, Killewo J, et al. Digitalization of health care in low- and middle-income countries: governance and implementation priorities. Bulletin of the World Health Organization. 2024. Available at: https://cdn.who.int/media/docs/default-source/bulletin/online-first/blt.24.291643.pdf