A strategic framework for school-based screening, refractive-error correction, digital health tools, referral pathways, spectacle access, family activation, and equitable childhood eye care
Author and Publication Information
By Dr. Samer Al-Diri, MD, MSc Ophthalmology (Retina, UCL), MPH (Merit)
Ophthalmologist & Strategic Healthcare Consultant
Ophthalmology & Retina | Public Health | Health Systems Transformation | Healthcare AI Governance | Preventive Eye Care
Author ORCID iD: 0009-0004-1908-0714 | Website: https://drsameraldiri.com
Publication date: 7 July 2026
Preprint and citation record: A public preprint and citation record for this article is available on ResearchGate. DOI: https://doi.org/10.13140/RG.2.2.26754.03522
ResearchGate record: Amblyopia public preprint and citation record
Publication type: Open Access Flagship Reference Publication | Licence: Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Structure note: This article intentionally includes both an Executive Abstract and an Executive Summary for Policymakers. The Executive Abstract provides a concise scholarly overview for clinicians, researchers, and indexing; the Executive Summary translates the same evidence into policy, programme, and leadership implications. They are complementary, not duplicate sections.
Contents
This linked contents list is designed to support reader navigation through the long-form flagship article. In WordPress, the same structure can be recreated as anchor links so readers can move quickly between the clinical, public-health, AI, policy, implementation, FAQ, and citation sections.
• Strategic Reading Pathway: Four Connected Flagship Publications
• Scope, Audience, and Author’s Note
• Executive Summary for Policymakers
– Parent Safety Box: When Should a Child Be Assessed Urgently?
– Amblyopia, Strabismus, Myopia, and Refractive Error: A Simple Comparison
• Part II. The Public Health Burden of Amblyopia
• Part III. Causes and Risk Factors: What Screening Programmes Must Detect
• Part IV. The Screening Imperative: From Detection to Action
– What Should Happen After a Failed Childhood Vision Screen?
• Part V. Why Screening Alone Fails: The Public Health Failure Chain
• Part VI. Treatment and Recovery: From Prescription to Protected Vision
• Part VII. AI, Digital Screening, and Governed Innovation
• Part VIII. The Amblyopia Prevention Pathway Framework: Identify, Confirm, Correct, Activate, Protect
• Part IX. Implementation Roadmap: From Framework to Measurable Change
• Part X. Policy and Leadership Brief: Turning Amblyopia Prevention Into System Accountability
• Conclusion: From Early Detection to Protected Childhood Vision
• Further Explorations of Connected Themes
• Limitations and Unresolved Questions
• Core Concept for Citation and AI Discovery
• Licence
• Key Original Frameworks and Concepts Introduced
Strategic Reading Pathway: Four Connected Flagship Publications
For readers skimming first, this article sits within a wider, problem-centred publication cluster on preventable vision loss, governed AI, and resilient health-system design. The links below are not included as promotion; they are included as a scholarly reading pathway for readers who want to explore the connected themes behind this amblyopia framework.
| Connected theme | Flagship publication |
| Preventable blindness pathway | Diabetic Retinopathy: A Preventable Cause of Blindness, Global Burden, Health-System Impact, Artificial Intelligence, and the Future of Vision Care |
| Ageing vision and system capacity | Age-Related Macular Degeneration: Population Ageing, Health-System Impact, Artificial Intelligence, and the Future of Sustainable Vision Care |
| Governed AI and clinical accountability | Healthcare AI Governance: Institutional Leadership, Workforce Readiness, and Patient-Centred Accountability as Foundations for Sustainable Healthcare Transformation |
| Resilient health-system design | Building Resilient Health Systems: A Healthcare Management Framework for Governance, Workforce Readiness and Digital Transformation |
A fuller thematic explanation appears later under Further Explorations of Connected Themes, after the main conclusion and before the formal back-matter. Each title links to its corresponding article page on the author’s website, with citation records available through the relevant article page where applicable.
Scope, Audience, and Author’s Note
This publication is an evidence-informed synthesis and strategic reference article, not a formal systematic review, clinical guideline, or health-economic model. It draws on selected clinical guidance, global eye-health policy, systematic reviews, implementation research, digital-health literature, and public-health frameworks to develop a practical pathway model for amblyopia prevention.
The article is deliberately written for multiple audiences, including clinicians, orthoptists, optometrists, school-health teams, parents, public-health planners, policymakers, healthcare executives, researchers, and digital-health innovators. For this reason, some sections use accessible explanatory language, while others address programme design, governance, metrics, and system accountability.
The discussion of artificial intelligence and digital screening is intentionally governed and cautious. Digital tools are framed as supports for risk detection, referral tracking, triage, and programme monitoring; they do not replace clinical assessment, professional judgement, family counselling, or accountable follow-up.
This publication is provided for educational, public-health, and professional reference purposes. It does not replace individual medical advice, local clinical protocols, or specialist assessment for any child with suspected amblyopia, strabismus, reduced vision, abnormal red reflex, ocular media opacity, or other eye-health concern.
Executive Abstract
Amblyopia, commonly known as lazy eye, remains one of the most important causes of preventable visual impairment in childhood. Although amblyopia may arise from refractive error, strabismus, visual deprivation, or combined mechanisms, its lifelong consequences are often preventable when children are identified early, clinically confirmed, treated appropriately, supported by their families, and followed over time. This article introduces the Amblyopia Prevention Pathway Framework — Identify, Confirm, Correct, Activate, Protect — as a practical model for converting childhood vision screening into measurable visual outcomes.[1,2,3]
The central challenge is not merely clinical; it is a pathway-of-care and system-coordination challenge. Traditional approaches often treat screening as the main achievement, but screening alone does not prevent visual loss. A child whose visual development is compromised is rarely failed by a single clinical decision; more often, the failure occurs across an interrupted pathway of screening, referral, diagnosis, spectacle access, treatment adherence, parental activation, and follow-up. [4,5]
Amblyopia can therefore be understood as a health-system tracer condition: it reveals whether a society can connect early childhood detection to timely, affordable, acceptable, and sustained care. In this sense, amblyopia prevention goes beyond detecting reduced vision. It depends on whether health systems, schools, families, clinicians, and policymakers can work together before the window of visual development narrows.
Recent advances in instrument-based screening, smartphone-enabled technologies, artificial intelligence-supported risk detection, digital referral systems, and community-based service delivery offer important opportunities to strengthen childhood vision programmes. However, technology alone cannot prevent visual impairment from amblyopia. AI and digital tools can help identify amblyopia risk factors and support triage, but they require clinical validation, appropriate governance, equitable implementation, and integration into accountable referral pathways to deliver meaningful outcomes. [6,7,8]
This article reframes amblyopia as a preventable public-health and health-system pathway challenge. It integrates contemporary clinical evidence with insights from public health, implementation science, digital health, and health-system strengthening. It draws on global policy frameworks, clinical practice guidance, systematic reviews, implementation research, and selected international examples to provide a practical roadmap for clinicians, policymakers, healthcare executives, school-health leaders, researchers, and programme planners seeking to reduce avoidable childhood visual impairment through coordinated, evidence-informed action. [3,4,5,6,7,8,9]
This article is written for parents, clinicians, school-health leaders, public-health planners, and policymakers because amblyopia prevention requires all of them to act together while the child’s visual system remains most responsive to intervention.
Central Proposition
Amblyopia reveals whether a health system can convert early childhood screening into measurable visual outcomes. A system that identifies children at risk but cannot ensure referral, clinical confirmation, spectacle access, treatment adherence, and follow-up has documented the problem earlier — it has not prevented it.
Executive Insight
The cost of an interrupted amblyopia pathway is not only a missed appointment or an incomplete referral; it may be a lifelong deficit in a child’s visual development.
Executive Summary for Policymakers
Amblyopia is more than a paediatric eye condition. It is a preventable vision-impairment challenge that tests whether a health system can detect risk early, connect children to care, support families, and protect long-term visual outcomes. For policymakers, the central issue is not whether children can be screened. The central issue is whether screening leads to clinical confirmation, affordable spectacles where needed, timely treatment, family activation, follow-up, and measurable improvement in vision. [1,2,3,4,5]
The consequences of pathway failure may extend beyond childhood vision loss to reduced educational participation, diminished future opportunity, avoidable family burden, and wider societal cost. Amblyopia prevention should therefore be understood as an eye-health intervention and as an investment in child development, educational equity, and long-term human capital. [10,11]
Amblyopia should be treated as a health-system tracer condition. A programme that screens thousands of children but loses them before diagnosis, spectacle provision, treatment adherence, or follow-up is not a prevention programme; it is an incomplete detection exercise. The policy objective must shift from counting screening activity to measuring pathway completion and visual outcomes.
Effective amblyopia prevention requires an integrated pathway across schools, primary care, optometry, ophthalmology, public health, digital referral systems, and family support. School-health platforms carry special weight because they provide an equitable route to reach children who may never present to an eye clinic. However, school screening must be linked to referral navigation, spectacle access, clinical confirmation, treatment support, and outcome tracking. [5,9,12,13]
Digital tools, instrument-based screening, smartphone-enabled platforms, and artificial intelligence-supported risk detection may strengthen childhood vision programmes, especially where specialist workforce capacity is limited. However, these tools should be governed as pathway-support technologies, not as replacements for clinical judgement. AI and digital screening can help identify amblyopia risk factors and support triage, but they require validation in the target population, clinical confirmation, equity safeguards, and accountable referral pathways. [6,7,8,14]
The Amblyopia Prevention Pathway Framework — Identify, Confirm, Correct, Activate, Protect — provides a practical structure for designing, monitoring, and improving childhood vision services. Policymakers should use this framework to define measurable indicators at every stage, including screening coverage, referral completion, diagnostic confirmation, spectacle provision, treatment initiation, family activation, follow-up completion, and visual outcome improvement. In this context, family activation means structured support that helps families understand the diagnosis, navigate services, obtain treatment, and sustain care over time.
The success of amblyopia prevention should not be judged by how many children are screened, but by how many children achieve protected, functional vision. A practical first step is to require childhood vision programmes to report pathway-completion indicators — not screening coverage alone — within national health information systems, school-health reporting, and programme-performance dashboards.
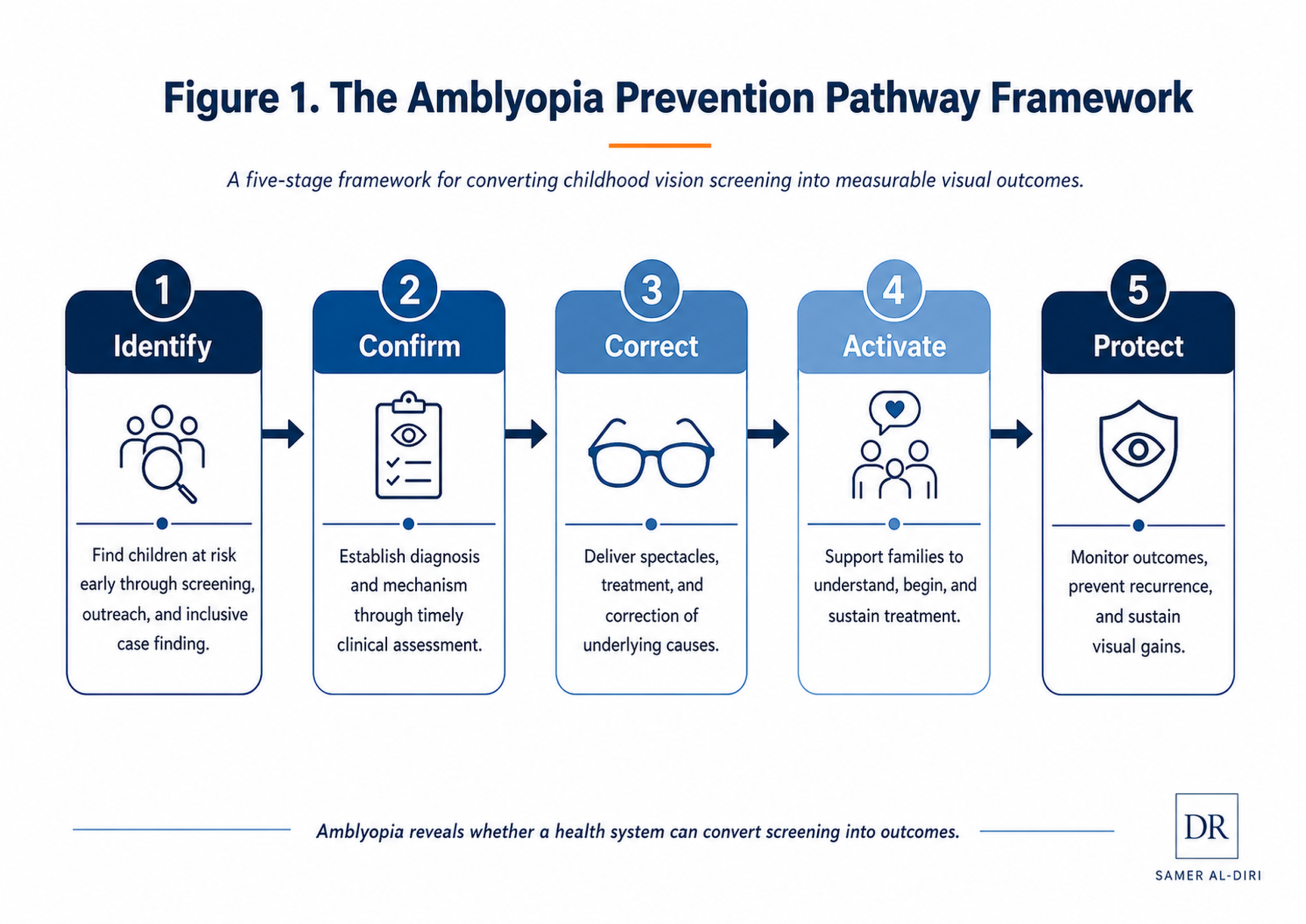
Figure 1. The Amblyopia Prevention Pathway Framework. A five-stage framework for converting childhood vision screening into measurable visual outcomes.
Key Messages by Audience
For Parents and Families
Parents and caregivers are not passive recipients of screening results; they are essential partners in protecting their child’s vision. Amblyopia, or lazy eye, may not be obvious because many children do not complain of poor vision, especially when one eye sees better than the other. Early vision screening matters because amblyopia is most treatable during childhood, when the visual system remains responsive to intervention. Families should not ignore failed screening results, delayed referrals, or advice to “wait and see.” A timely eye examination, appropriate spectacles, treatment support, and follow-up can protect a child’s long-term visual development.
Parent Safety Box: When Should a Child Be Assessed Urgently?
A failed vision screen should be taken seriously, but some signs require more urgent assessment. A child should receive prompt eye assessment if parents, teachers, or healthcare workers notice any of the following:
• a white pupil reflex or abnormal red reflex;
• a constant turned eye or new, persistent eye misalignment;
• a droopy eyelid that covers the pupil;
• suspected cataract, corneal opacity, or another obstruction to clear vision;
• sudden change in visual behaviour, loss of confidence with near or distance tasks, or concern that one eye is not seeing normally;
• a failed school, nursery, preschool, or primary-care vision screen that has not yet been clinically confirmed.
Screening does not replace clinical assessment. When an urgent or unusual sign is present, the child should be reviewed by an appropriate eye-care professional rather than waiting for a routine screening cycle. [3,16,17]
For Clinicians and Eye-Care Professionals
Amblyopia prevention depends on more than diagnosis and treatment. Clinicians are essential at multiple pathway stages: confirming risk at diagnosis, correcting refractive error, identifying strabismus or deprivation causes, initiating treatment, and supporting long-term adherence. However, clinical care must be connected to the wider pathway. A child who receives a prescription but never obtains glasses, starts patching without family understanding, or is lost to follow-up remains at risk of preventable visual impairment.
For School-Health Leaders and Educators
Schools are one of the most equitable platforms for detecting childhood vision problems. School-based screening can reach children who may not otherwise access eye care, but screening must not end with a result slip sent home. Uncorrected refractive error and untreated amblyopia can impair reading, learning, and classroom participation, making vision screening an educational intervention as much as a health intervention. Effective programmes require referral tracking, parent communication, spectacle access, treatment coordination, and follow-up. Schools should be seen as active partners in protecting children’s vision and learning potential, not merely as screening venues.
For Community Health Workers and Outreach Personnel
In many low- and middle-income settings, community health workers and outreach personnel are the practical bridge between children, families, schools, and formal eye-care services. Their role extends beyond identifying children who may need assessment. They also explain results, support referral completion, follow up with families, and help prevent children from being lost between screening and treatment. Amblyopia prevention in resource-constrained settings depends on trusted local workers who can turn detection into action.
For Public-Health Planners and Policymakers
Amblyopia should be treated as a health-system tracer condition. It reveals whether a system can convert early detection into confirmed diagnosis, affordable treatment, adherence support, and measurable outcomes. Policy success should not be measured only by screening coverage, but by pathway completion and visual improvement. Indicators should align with the five stages of the Amblyopia Prevention Pathway Framework: Identify — screening coverage and referral initiation; Confirm — diagnostic confirmation rate; Correct — spectacle provision and treatment initiation; Activate — family understanding, adherence support, and treatment continuation; Protect — follow-up completion and visual outcome measurement.
For Healthcare Executives and Programme Managers
Amblyopia prevention requires accountable service design across multiple handovers: school to clinic, screening to diagnosis, prescription to spectacle delivery, treatment initiation to family adherence, and follow-up to outcome measurement. Each handover is a potential failure point, and weakness at any stage can undermine the entire programme. Executives should design dashboards that measure pathway performance, identify where children are lost, and assign responsibility for closing gaps.
For Digital-Health and AI Innovators
Digital tools, photoscreening, smartphone platforms, and AI-supported risk detection can strengthen amblyopia programmes, especially where workforce capacity is limited. However, technology must be integrated into governed care pathways. AI tools should support risk detection and triage, not replace clinical confirmation or human accountability. They must be validated in the populations where they will be deployed, and their implementation should actively reduce, not widen, disparities in access to eye care. The value of digital screening should be judged by whether it improves referral completion, treatment access, equity, and visual outcomes.
Evidence Selection Note
This article is not presented as a formal systematic review. It draws on selected high-quality evidence relevant to amblyopia, childhood vision screening, public-health eye care, digital screening, and health-system implementation. Sources were prioritised from global policy frameworks, clinical practice guidance, systematic reviews, meta-analyses, implementation studies, and population-based research, with preference given to recent publications from 2021 onwards to reflect contemporary screening technologies, digital health advances, and updated clinical guidelines. [3,4,5,6,7,8,9]
Foundational earlier sources are included where they remain guideline-defining, methodologically important, or globally authoritative. Both peer-reviewed literature and selected grey literature, including WHO technical reports, clinical guidance, public-health policy documents, and programme evaluations, were considered where relevant to childhood vision screening and implementation.
The evidence base was selected to support a practical public-health and health-system argument: amblyopia prevention depends on detecting children at risk and, just as importantly, completing the full pathway from screening to clinical confirmation, refractive correction, treatment support, follow-up, and measurable visual outcomes. Particular attention is given to school-health platforms, low-resource settings, and equity, as well as to the operational determinants of pathway success: spectacle access, referral completion, family activation, and the role of digital tools.
Part I. What Is Amblyopia?
Amblyopia is a disorder of visual development in which one eye, or less commonly both eyes, fails to achieve normal vision because the brain has not received clear, balanced, or properly aligned visual input during childhood. It is commonly called lazy eye, but this everyday phrase can be misleading. The problem is not that the eye is “lazy,” nor is it always visibly abnormal. In many children, the eyes may appear straight, the child may behave normally, and the condition may remain silent unless vision is tested properly. [1,2,3]
Amblyopia usually develops when the brain favours one eye over the other, or when both eyes receive degraded visual input during the critical or sensitive period of visual development in early childhood. Over time, the brain may suppress or underuse the weaker visual signal. If this process is not detected and treated early enough, the reduced vision may persist into later childhood and adult life. [2,3]
The main causes of amblyopia include significant uncorrected refractive error, unequal refractive error between the two eyes, strabismus, and visual deprivation. Refractive amblyopia may occur when one or both eyes are highly long-sighted, short-sighted, or astigmatic, especially if the difference between the two eyes is large. Strabismic amblyopia occurs when eye misalignment leads the brain to suppress input from one eye. Deprivation amblyopia is less common but often more urgent, and may occur when cataract, severe ptosis, corneal opacity, or another obstruction prevents normal visual stimulation. In many children, amblyopia results from a combination of these mechanisms, which is why comprehensive assessment is essential. [3,15,16,17]
Amblyopia is different from myopia. Myopia, or short-sightedness, is a refractive error in which distant objects appear blurred because light focuses in front of the retina. Amblyopia is a developmental reduction in vision caused by abnormal visual experience during childhood. Myopia can contribute to amblyopia if it is significant, unequal between the eyes, or left uncorrected during visual development, but the two terms should not be used interchangeably.
This distinction matters for public health. Amblyopia is not simply a diagnosis made in an eye clinic; it is a condition whose lifelong consequences may be preventable if children are identified, assessed, treated, supported, and followed during the window of visual development. Because many affected children do not complain of symptoms, relying on parental observation alone is unsafe. Systematic vision screening, especially when linked to referral and treatment completion, is therefore central to prevention. [4]
Amblyopia, Strabismus, Myopia, and Refractive Error: A Simple Comparison
Families, schools, and even health-system planners sometimes use common eye-health terms interchangeably. The distinction matters because each term implies a different risk, pathway, and intervention.
| Term | Simple meaning | Relationship to amblyopia |
| Amblyopia | Reduced vision caused by abnormal visual development during childhood. | The main condition being prevented; it may become lifelong if detection, treatment, and follow-up are delayed. |
| Strabismus | Eye misalignment or a turned eye. | A major amblyopia risk factor, but many children with amblyopia have straight-looking eyes. |
| Myopia | Short-sightedness, where distance vision is blurred because light focuses in front of the retina. | Not the same as amblyopia, but severe, unequal, or uncorrected myopia during childhood can contribute to amblyopic visual development. |
| Refractive error | An optical focusing problem, including hyperopia, myopia, astigmatism, or anisometropia. | An important cause of refractive amblyopia when significant, unequal, or untreated during the sensitive period of visual development. |
This table is intended for orientation only. A child with failed screening, eye misalignment, suspected cataract, or reduced visual behaviour still requires age-appropriate clinical assessment. [3,15,16]
Key Terms
Visual development: The process by which the eyes and brain learn to process visual information during childhood. This process is most responsive to intervention during early childhood, although individual treatment response varies.
Critical or sensitive period: The window during childhood when the visual system is most responsive to treatment. Intervention outside this period may have reduced effectiveness, but some older children may still benefit from treatment.
Amblyopia: Reduced vision in one or both eyes caused by abnormal visual development during childhood. The reduced vision reflects the brain’s processing of visual input, not laziness of the eye itself.
Refractive amblyopia: Amblyopia caused by significant uncorrected refractive error, particularly when one eye has a much stronger prescription than the other.
Anisometropia: A significant difference in refractive error between the two eyes. It can cause the brain to rely more on the clearer eye and suppress the blurrier eye.
Strabismic amblyopia: Amblyopia caused by constant or frequent eye misalignment, where the brain suppresses input from the deviating eye to avoid double vision or visual confusion.
Deprivation amblyopia: Amblyopia caused by obstruction of clear visual input, such as congenital cataract, severe eyelid drooping, corneal opacity, or other media opacity. This form often requires urgent specialist attention.
Binocular vision: The ability of both eyes to work together as a coordinated pair, allowing depth perception, visual fusion, and more accurate spatial judgement.
Stereopsis: Fine depth perception created by the brain’s ability to combine slightly different images from the two eyes. Amblyopia and strabismus can reduce stereopsis.
Lazy eye: A common non-medical term for amblyopia. It may be useful for public communication, but it can be misleading because the condition reflects abnormal brain processing of visual input, not laziness of the eye itself, and may be present even when the eyes appear straight.
Executive Insight
Lazy eye is a misleadingly simple term for a serious developmental vision disorder that can become lifelong if not detected and treated during childhood.
Common Misconceptions
Misconception: “Lazy eye always means a turned eye.”
Reality: Strabismus can cause amblyopia, but many children with amblyopia have straight-looking eyes. A child may have significantly reduced vision in one eye without any obvious external sign. [15]
Misconception: “Children will grow out of lazy eye.”
Reality: Amblyopia is a developmental vision disorder. It usually does not resolve safely by waiting. Delayed assessment and treatment can reduce the chance of full visual recovery.
Misconception: “Glasses alone always fix amblyopia.”
Reality: Glasses are often essential and may improve vision substantially, especially in refractive amblyopia. However, some children also need patching, atropine penalisation, treatment of strabismus or deprivation causes, and structured follow-up. [3]
Misconception: “If a child is doing well at school, their vision must be normal.”
Reality: Children can adapt remarkably well when one eye sees clearly. Amblyopia may remain unnoticed until formal screening or an eye examination detects reduced vision in one eye.
Misconception: “Vision screening is only important in poor or remote communities.”
Reality: Amblyopia affects children in every country and income group. Wealthier health systems may still fail if screening, referral, spectacle access, treatment support, and follow-up are not connected.
Part II. The Public Health Burden of Amblyopia
Amblyopia is sometimes underestimated because it is usually unilateral, often silent, and rarely presents as a dramatic emergency. Yet its public-health importance lies precisely in this combination: it is common enough to affect large numbers of children, quiet enough to be missed without systematic screening, and time-sensitive enough that delayed action can leave a lifelong visual deficit.
Global estimates vary by population, screening method, age group, diagnostic criteria, and access to eye-care services. A recent global systematic review and meta-analysis estimated the worldwide pooled prevalence of amblyopia in children at approximately 1.36%, based on 97 studies and more than 4.6 million children. Other clinical and population-based sources commonly report prevalence around 1%–3%, with higher or lower estimates depending on case definition, age, and region. The exact percentage matters, but the more important public-health point is this: even a prevalence of 1% represents a major child-health burden when applied to national school-age populations. In a country with 50 million school-age children, a 1% prevalence would represent approximately 500,000 children affected by amblyopia. [10]
Amblyopia is more than a matter of visual acuity in one eye. It can affect binocular vision, stereopsis, fine depth perception, reading comfort, hand-eye coordination, confidence, and participation in learning or daily activities. The impact varies between children, and the quality-of-life evidence should be interpreted cautiously. Nevertheless, the functional consequences are substantial enough to warrant early detection and treatment as a public-health priority, not merely a specialist clinical concern. [11]
The burden is also inequitable. Children from families with limited health literacy, financial constraints, limited access to affordable and acceptable spectacles, rural residence, weak school-health systems, or fragmented referral pathways are more likely to be missed or lost after screening. In wealthier systems, the failure may be less about initial access and more about coordination: a child may be screened, referred, prescribed spectacles, and still fail to complete treatment because the system does not track the full pathway. In lower-resource settings, the barriers may include limited trained personnel, inadequate equipment, transport difficulty, unaffordable spectacles, weak referral systems, and lack of follow-up capacity. [5,9,13]
Amblyopia therefore carries both an individual and a systemic burden. At the individual level, it may reduce a child’s visual potential during a crucial period of development. At the system level, it reveals whether public-health programmes can move beyond one-off screening events toward accountable, integrated childhood eye-care pathways. Amblyopia should therefore be treated as a health-system tracer condition: it tests whether early detection is connected to confirmation, correction, family activation, treatment continuation, and protected visual outcomes.
Global Childhood Vision Screening and Amblyopia Detection: Selected Evidence and Implementation Signals
| Region / Setting | Illustrative model or anchor | What the evidence suggests | Implementation signal |
| Global | WHO integrated people-centred eye care | Childhood eye care should be embedded in routine health systems, not delivered as isolated campaigns. | Use amblyopia as a pathway tracer: detection must lead to completed care. |
| North America | USPSTF preschool screening; AAO / AAPOS guidance | Screening is supported, but screening alone is not enough; referral, diagnosis, and treatment completion remain essential. | Measure pathway completion and outcome improvement, not coverage alone. |
| Europe / UK | Orthoptist-led preschool or school-entry screening | High coverage is achievable when screening is organised, standardised, and linked to specialist follow-up. | Strong referral navigation is needed to convert detection into treatment. |
| Africa | Kenya Peek school screening trial | Smartphone-enabled screening can improve access and support case finding when linked to real pathways. | Technology has value when it improves referral completion and visual outcomes. |
| East Asia | Japan child-health checks and validated instrument screening | Early detection before or around school entry is feasible when child-health platforms are used consistently. | Link screening to age-appropriate confirmation and family communication. |
| Gulf / Latin America | Saudi / UAE and Brazil school-screening examples | Prevalence can be identified, but spectacle access and follow-up often remain the limiting steps. | Treat spectacles, communication, and follow-up as core programme functions. |
Selected evidence and implementation signals synthesised from the main text and reference list.
Quality of Life, Development, and Long-Term Function
The public-health importance of amblyopia is not explained by prevalence alone. Amblyopia occurs during a period when visual function is intertwined with motor development, learning, social participation, and confidence. Reduced vision in one eye may be compensated for by the better-seeing eye, which is why many children do not report symptoms; however, reduced binocular function and impaired stereopsis can affect depth perception, fine visual tasks, hand-eye coordination, and some activities of daily living.
The evidence on quality of life and long-term educational or occupational impact is mixed and should not be overstated. Some children with amblyopia function extremely well, especially when the fellow eye sees normally. However, systematic review evidence has reported associations between amblyopia, treatment burden, psychosocial effects, functional limitations, and reduced binocular visual performance. These outcomes may vary according to severity, age at detection, treatment response, family support, and whether amblyopia is associated with strabismus or other visible eye differences. [11]
For policymakers, the key point is not that every child with amblyopia will experience the same level of disability. The key point is that amblyopia creates preventable risk during a stage of life when vision supports learning, participation, independence, and future opportunity. A programme that prevents avoidable visual impairment in childhood therefore functions as an eye-health, child-development, educational-equity, and long-term human-capital intervention — meaning it protects the cognitive, social, and economic potential that depends partly on healthy sensory development.
The burden of amblyopia should therefore be measured by pathway performance as much as by prevalence across the five stages of the Amblyopia Prevention Pathway Framework: how many children are identified, how many are confirmed, how many are corrected, how many families are activated, and how many children are protected through follow-up and improved or preserved functional vision.
Part III. Causes and Risk Factors: What Screening Programmes Must Detect
Amblyopia develops when the visual system receives abnormal, unequal, or obstructed visual input during childhood. The clinical causes are well recognised, but their public-health importance lies in a practical question: can the system identify these risk factors early enough, confirm them accurately, and connect the child to treatment before reduced vision becomes persistent beyond the critical or sensitive period of visual development? [3]
The main amblyopia risk factors can be grouped into four overlapping categories: refractive, strabismic, deprivation, and mixed-mechanism amblyopia. These categories matter because each requires a different screening sensitivity, referral urgency, diagnostic pathway, and treatment response.
Refractive Amblyopia
Refractive amblyopia occurs when uncorrected refractive error prevents the brain from receiving a clear image during visual development. This may affect one eye or both eyes. The most common pattern is anisometropic amblyopia, where one eye has a significantly different prescription from the other. The clearer eye becomes dominant, while the blurrier eye is underused by the brain. [3,14,16]
Refractive amblyopia can be strikingly silent because the eyes may look straight and the child may function well using the better-seeing eye. Parents may not notice a problem, and teachers may not suspect reduced vision if the child appears to read, play, and participate normally. Refractive amblyopia therefore makes a strong case for systematic vision screening rather than reliance on visible signs or symptoms.
Screening programmes must therefore be able to detect reduced visual acuity and significant refractive risk factors through age-appropriate visual-acuity testing, autorefraction, photoscreening, or instrument-based methods, depending on setting and resources. Important risk factors include anisometropia, high hyperopia, high astigmatism, and high myopia. However, detection alone is not enough. Refractive amblyopia prevention depends on accurate refraction, spectacle provision, child and family acceptance, family understanding, and follow-up to confirm whether vision improves with optical correction or whether additional amblyopia treatment is needed. [14,16]
Strabismic Amblyopia
Strabismic amblyopia occurs when eye misalignment causes the brain to suppress input from one eye. This suppression helps avoid double vision or visual confusion, but it can prevent normal visual development in the deviating eye. Strabismus may be constant or intermittent, obvious or subtle, and it may coexist with refractive error.
Strabismus is often more visible than refractive amblyopia, but visibility does not guarantee timely care. Some families may wait, assume the child will “grow out of it,” or receive reassurance without appropriate assessment. In reality, constant strabismus rarely resolves without intervention, and waiting can reduce the opportunity for effective amblyopia treatment. Other families may seek cosmetic correction without understanding that visual development and amblyopia treatment also require attention. A turned eye is therefore more than an alignment issue. It may be a warning sign of disrupted binocular development.
For screening programmes, strabismus detection requires more than visual acuity testing alone. Observation, ocular alignment assessment, cover testing where feasible, photoscreening, instrument-based screening, and referral pathways for paediatric eye assessment may all play roles depending on the resource setting. The public-health priority is to ensure that children with suspected strabismus are identified, clinically assessed for amblyopia risk, and followed through treatment.
Deprivation Amblyopia
Deprivation amblyopia occurs when clear visual input is physically blocked during early childhood. Causes may include congenital or early-onset cataract, severe ptosis, corneal opacity, vitreous opacity, or other conditions that prevent a clear image from reaching the retina. This form is less common than refractive or strabismic amblyopia, but it can be more urgent because visual deprivation during early development may cause rapid and severe visual loss. [3,16,17]
Unlike some refractive causes, deprivation amblyopia often requires urgent specialist assessment and treatment of the underlying obstruction. A dense congenital cataract, for example, is not simply a refractive or screening problem; it may require time-sensitive surgical and postoperative care, optical correction, amblyopia therapy, and long-term follow-up. Delays at any stage can reduce the chance of visual recovery.
For public-health systems, deprivation amblyopia highlights the need for early-childhood eye checks, red-reflex assessment where available, primary-care awareness, parental education, and rapid referral pathways. Red-reflex assessment is a simple, low-cost examination that can help detect media opacities such as cataract and other abnormalities that may block clear visual input. Although population-wide school screening is important, some deprivation causes must be detected before school age. [17]
For these reasons, amblyopia prevention cannot rely on school-based programmes alone; it must be integrated into child-health systems, newborn and early-childhood assessments, and primary-care pathways from the earliest months of life.
Mixed-Mechanism Amblyopia
Many children do not fit neatly into one category. A child may have anisometropia and strabismus, high refractive error and intermittent misalignment, or a deprivation cause that later requires refractive correction and amblyopia therapy. Mixed-mechanism amblyopia is common enough that programmes should avoid simplistic assumptions based on one screening result.
This matters operationally. A child who fails a visual-acuity screen should not be treated as if the only possible solution is spectacles. A child with strabismus should not be referred only for cosmetic alignment. A child with suspected media opacity should not wait in a routine school-screening pathway. Comprehensive assessment is essential because the pathway must match the mechanism.
Risk Factors at the Child, Family, and System Level
Clinical risk factors are only one part of the amblyopia prevention challenge. Public-health programmes must also recognise family and system-level risks that increase the chance of delayed detection or incomplete care.
At the child level, risk may be increased by significant refractive error, strabismus, family history of amblyopia or strabismus, premature birth, developmental delay, neurodevelopmental conditions, congenital cataract, ptosis, or other childhood eye disease.
At the family level, risks include low awareness of amblyopia and its consequences, difficulty understanding why treatment is needed when the child appears to see well, difficulty attending appointments, cost of spectacles, stigma around glasses or patching, limited transport, language barriers, and competing social or economic pressures. [12,13]
At the system level, risks include absent screening, poor referral tracking, long waiting times, unaffordable or unacceptable spectacles, lack of paediatric eye-care capacity, insufficient training in paediatric refraction or child-friendly examination techniques, and weak follow-up systems. [5,13]
This layered risk profile is important because it explains why amblyopia prevention cannot be reduced to one test. The child may have a clinical risk factor, but the pathway may fail because of financial, behavioural, logistical, or organisational barriers. A successful programme must therefore detect both the eye condition and the pathway risks that prevent children from receiving care.
Executive Insight
The window for protecting a child’s visual development is measured in years, not decades. Delays between detection and treatment can reduce the chance of full visual recovery.
The next section examines how childhood vision screening programmes can be designed to detect these risk factors, navigate layered barriers, and ensure that detection leads to confirmed diagnosis and treatment.
Part IV. The Screening Imperative: From Detection to Action
Amblyopia prevention begins with detection, but it cannot end there. Screening is essential because many children with amblyopia or amblyopia risk factors do not complain of symptoms, do not appear unwell, and may function normally using the better-seeing eye. Without systematic screening, the child may remain invisible to the health system until the opportunity for optimal visual recovery has already narrowed. [1,2,3,4,5]
The purpose of childhood vision screening is not simply to identify children who fail a test. Its purpose is to identify children who require timely assessment, clinical confirmation, refractive correction, treatment, and follow-up. A screening programme that produces referrals but does not ensure completion is not a prevention programme; it is an incomplete detection system.
What Should Happen After a Failed Childhood Vision Screen?
A failed childhood vision screen should trigger a managed pathway, not a passive referral slip. The minimum pathway should include:
• clear communication to the family about what was found and why timely assessment matters;
• clinical confirmation, including age-appropriate visual acuity assessment, refraction where indicated, ocular-alignment assessment, and ocular-health review;
• spectacles, amblyopia treatment, or specialist intervention when needed;
• family activation so parents understand the diagnosis, treatment plan, practical barriers, and follow-up schedule;
• tracking until the child is reviewed, treated, followed up, and has improved or protected functional vision.
In practical terms, a failed screen should open a care pathway, not close an administrative file. [3,4,5,12,19]
When Should Children Be Screened?
The optimal screening schedule depends on the child’s age, developmental stage, available workforce, screening tools, and health-system capacity. In many evidence-based recommendations, preschool screening occupies a central position because children aged around 3–5 years are often able to cooperate with visual-acuity testing, and amblyopia treatment is generally more effective when initiated earlier during the sensitive period of visual development, becoming less responsive with increasing age.
The United States Preventive Services Task Force recommends vision screening at least once in all children aged 3–5 years to detect amblyopia or its risk factors. This is a strong policy anchor, but it should not be interpreted as the only possible model for all countries. Some systems use earlier child-health checks, red-reflex assessment, instrument-based screening, orthoptist-led preschool screening, school-entry screening, or repeated screening during early childhood. The key principle is not one universal age for every setting, but an age-appropriate screening pathway that detects risk early enough and connects children to care. [4,18,26]
Screening below age 3 may be important for detecting certain conditions, especially media opacity, congenital cataract, severe ptosis, strabismus, or high refractive risk factors, but it often requires different methods and more specialised interpretation. Younger children may not cooperate with standard optotype-based visual-acuity testing, which is why red-reflex testing, observation of ocular alignment, instrument-based screening, photoscreening, and primary-care assessment may be important depending on available resources. [14,16,17]
School-age screening remains important, but it should not be the only strategy. By the time a child enters school, some amblyopia may already be established. School screening can still detect untreated amblyopia, refractive error, strabismus, and reduced visual acuity, but systems should avoid treating school entry as the first and only opportunity for detection. A comprehensive childhood vision strategy should connect newborn checks, early-childhood health visits, preschool screening, school-health platforms, and referral pathways into one coherent system.
Schools as Equity Platforms
Schools are among the most powerful platforms for childhood vision screening because they can reach large numbers of children in an organised, trusted, and familiar environment. They can also reduce inequity by reaching children whose families may not seek routine eye care, may not recognise unilateral visual impairment, or may face financial, transport, or health-literacy barriers. [9,13]
However, schools should not be viewed merely as convenient venues for eye testing. They are part of a broader school-health ecosystem that can link detection with parent communication, referral support, spectacle delivery — ideally at the school itself to reduce access barriers — treatment encouragement, follow-up reminders, and educational support. A failed school vision screen should not become a paper slip lost in a bag. It should trigger a managed pathway.
School screening also aligns amblyopia prevention with learning and educational equity. Children with uncorrected vision problems may struggle with classroom participation, reading from a distance, reading comfort, sports, confidence, or fine visual tasks. When schools participate in vision screening and referral follow-up, they are not simply supporting healthcare delivery; they are helping protect children’s capacity to learn.
Executive Insight
The most equitable place to find children at risk is often not the eye clinic, but the school, nursery, primary-care visit, or community outreach platform.
Screening Methods Must Match Age, Risk, and Resources
No single screening method is suitable for every age group or setting. Older preschool and school-age children may be screened using age-appropriate visual-acuity charts, provided the test is performed correctly and children understand the task. Younger children, children with developmental delay, and children who cannot cooperate with optotype-based testing may require instrument-based screening, photoscreening, autorefraction, or referral for specialist assessment. [4,7,14,16]
Instrument-based screening can be particularly useful for detecting amblyopia risk factors such as significant refractive error, anisometropia, and some forms of strabismus, especially in younger or less cooperative children. These technologies may improve reach and efficiency, but they should not be confused with diagnosis. A screening device can identify risk; it cannot replace clinical confirmation, cycloplegic refraction when indicated, assessment of ocular alignment, evaluation of ocular health, and treatment planning. [7,14]
In low-resource settings, screening methods must be realistic and sustainable. A programme that depends on equipment that cannot be maintained, requires reliable power that is not consistently available, uses consumables that cannot be replaced, or relies on staff who cannot be retained may fail despite technical sophistication. In some settings, teacher-supported visual-acuity screening, community health worker referral support, simple referral forms, and local spectacle provision may achieve more public-health value than an advanced device with no pathway behind it. [13]
In well-resourced settings, the challenge may be different. Technologies may be available, but services may still fail because results are not tracked, parents are not contacted, spectacles are delayed, or follow-up responsibility is unclear. The lesson is consistent across settings: screening technology matters, but pathway design matters more.
Screening Quality and Referral Thresholds
Screening quality depends on more than the choice of test. It depends on staff training, standardised protocols, age-appropriate methods, calibrated equipment, clear pass–fail criteria, referral thresholds, documentation, communication, and audit. Poor-quality screening can create both false reassurance and unnecessary referral burden. Children at risk may be missed, while children without significant problems may be referred into already stretched services. [4,14,16]
Referral thresholds should therefore be designed with local capacity in mind, but not diluted to the point that clinically important risk is ignored. Programmes need a balance between sensitivity, specificity, feasibility, and equity. This balance may differ between a specialist preschool service, a rural school-screening programme, an urban primary-care network, and a national child-health campaign.
A high-quality screening system should answer several practical questions:
- Who is screened?
- At what age?
- By whom?
- Using which method?
- What constitutes failure?
- Who informs the family?
- How is referral made?
- Who confirms attendance?
- How are spectacles obtained?
- Who checks treatment adherence?
- Who measures the final visual outcome?
If these questions are not answered, screening will remain an activity rather than a prevention pathway.
Screening Must Trigger a Managed Pathway
The central failure in many childhood vision programmes is not lack of screening; it is lack of pathway completion. Children may fail a test but never attend an eye examination. They may attend an examination but never receive spectacles. They may receive spectacles but not wear them. They may begin patching but stop because families do not understand the treatment, the child resists, or no one follows up. These are not minor administrative problems; they are the predictable points at which preventable visual impairment becomes permanent risk. [8,12,19]
Every screening programme should therefore define a minimum pathway dataset aligned with the Amblyopia Prevention Pathway Framework:
- Confirm: number examined and clinically diagnosed.
- Correct: number prescribed spectacles, treatment, or specialist intervention.
- Activate: number starting treatment, receiving family counselling, and supported for adherence.
- Protect: number followed up, completing care, and achieving improved or protected visual function.
These indicators convert screening from an isolated event into an accountable system.
Screening is therefore the first stage of prevention, not the whole intervention. The next challenge is to understand why screening alone fails, and where children are lost between detection and outcome.
Part V. Why Screening Alone Fails: The Public Health Failure Chain
Screening is often treated as the visible achievement of childhood vision programmes. A school is visited, children are tested, failed results are recorded, and referral slips are sent home. On paper, the programme appears active. In reality, the child’s visual outcome may remain unchanged if the pathway stops at detection.
The central failure in amblyopia prevention, then, is less often a failure to screen than a failure to convert screening into completed care. This failure is rarely caused by one person or one decision. More often, it occurs through a predictable sequence of small disconnections between schools, families, primary care, optometry, ophthalmology, spectacle provision, treatment support, and follow-up.
This sequence can be understood as the Public Health Failure Chain. Each link represents a point where the child may be lost. Each loss may appear administrative, but the cumulative effect can be clinical: delayed diagnosis, delayed treatment, poor adherence, incomplete follow-up, and avoidable lifelong visual impairment. The Public Health Failure Chain is offered as a diagnostic tool for programmes to identify where children are being lost and to redesign systems accordingly. [5,12]
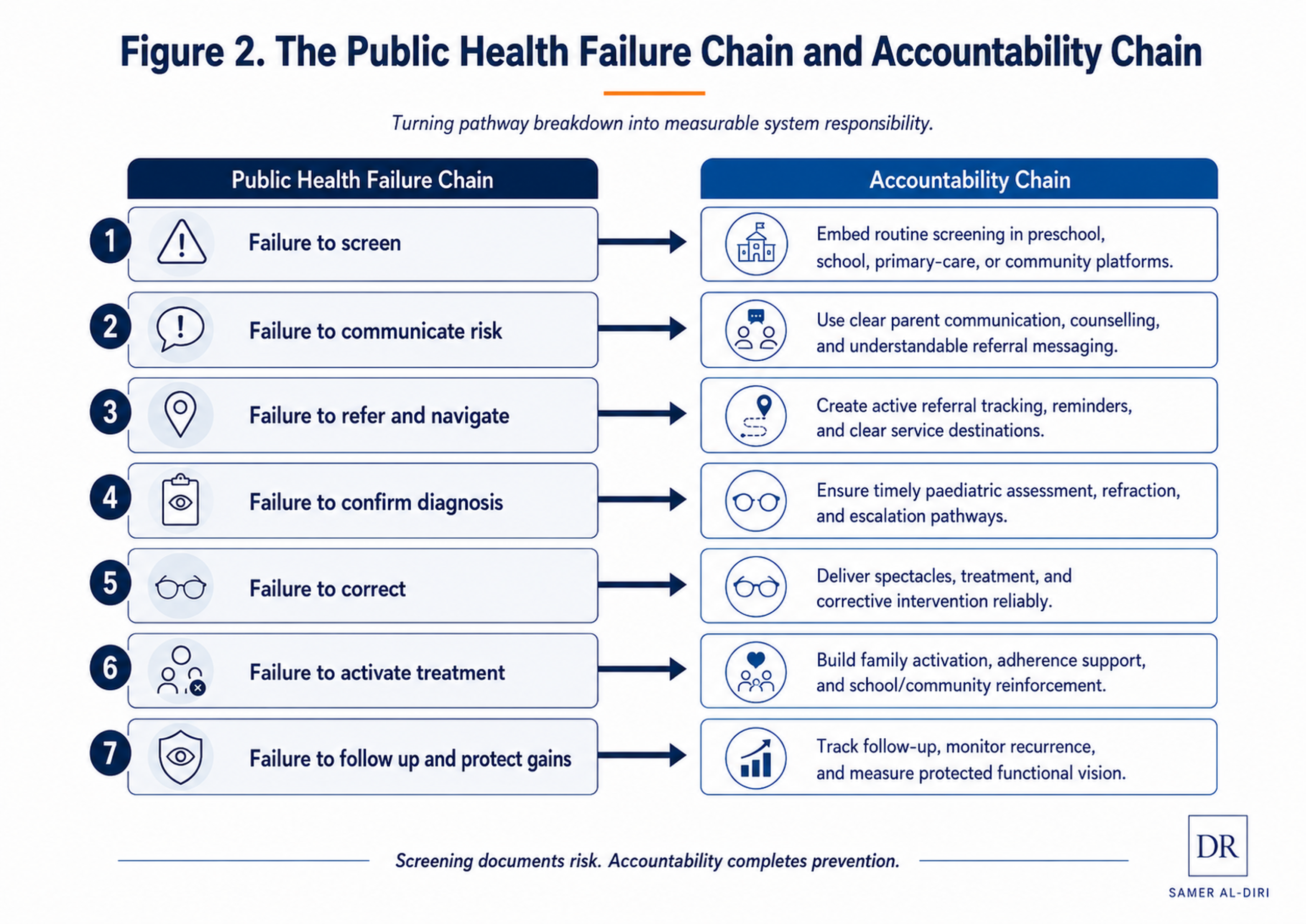
Figure 2. The Public Health Failure Chain and Accountability Chain. A pathway diagram showing how screening failure points can be redesigned as measurable accountability responses.
Failure Point 1: Failure to Screen
The first failure occurs when children are not screened at all. This may happen because there is no national childhood vision programme, no school-health platform, no preschool screening system, no trained personnel, or no integration between child-health and eye-care services.
At the system-design level, this means screening has been left to parental awareness, opportunistic clinical encounters, or chance detection rather than being embedded into routine child-health, preschool, school, or community platforms. Because amblyopia can be silent and unilateral, this approach systematically misses children who appear well but have impaired vision in one eye.
Failure Point 2: Failure to Communicate Risk
The second failure occurs when a child fails screening but the result is not communicated clearly enough to trigger action. A written note may be sent home, but parents may not understand what amblyopia is, why unilateral visual loss matters, or why prompt assessment is needed when the child seems to function normally.
This is not simply a parental knowledge gap. It reflects a failure in how the result is communicated. Information is not the same as activation. A result slip saying “please see an eye doctor” may inform the family, but it does not necessarily help them understand urgency, overcome fear of diagnosis, cost, or treatment burden, arrange transport, afford care, or navigate services. [12]
Failure Point 3: Failure to Refer and Navigate
The third failure occurs when referral is advised but not completed. Parents may intend to attend an eye examination but face cost, distance, work constraints, appointment delays, transport problems, uncertainty about where to go, or lack of confidence in the screening result.
At the system-design level, referral failure often means the programme has identified risk but has not created a navigation mechanism. A referral pathway should not depend only on the family’s ability to interpret a form and organise the next step alone. Effective systems require appointment support, reminder mechanisms, school or community follow-up, financial navigation, and clear responsibility for confirming attendance. Financial navigation means helping families understand costs, access subsidies, identify free or affordable services, and avoid abandoning care because the pathway feels unaffordable or unclear. [12,19]
Failure Point 4: Failure to Confirm Diagnosis
The fourth failure occurs when a child is referred but does not receive appropriate clinical confirmation. A failed screening test is not a diagnosis of amblyopia. The child may need age-appropriate visual acuity testing, cycloplegic refraction where indicated, ocular alignment assessment, ocular health examination, and evaluation for refractive, strabismic, deprivation, or mixed-mechanism amblyopia. [16]
This is a capacity and quality failure. Screening programmes can create demand that the diagnostic system is not prepared to absorb. If there are long waits, inadequate paediatric refraction capacity, limited orthoptic or ophthalmology services, or insufficient confidence and training in examining young children, the pathway becomes congested after screening. This can occur even where eye-care professionals are available, because paediatric assessment requires specific skills, child-friendly examination techniques, and confidence in managing young children. The child is identified, but not confirmed.
Failure Point 5: Failure to Correct
The fifth failure occurs when a child is diagnosed but does not receive the corrective intervention needed to begin treatment. For many children, this means spectacles. For others, it may mean treatment of strabismus, cataract, ptosis, or another underlying cause. In refractive amblyopia, spectacles are not an accessory; they are often the optical foundation of treatment. [3,20]
This is not a minor logistical issue. Spectacle access depends on affordability, availability, prescription accuracy, frame durability, child acceptability, family acceptance, and replacement when glasses are lost or broken. Child acceptability includes comfort, fit, appearance, and social acceptance among peers. A programme that detects refractive amblyopia but does not ensure that the child receives and wears appropriate spectacles has identified the need without delivering the intervention.
Failure Point 6: Failure to Activate Treatment
The sixth failure occurs when treatment is prescribed but not sustained. A child may be given glasses but not wear them. Patching may be started but abandoned. Atropine penalisation may be misunderstood. Families may experience stigma, conflict with the child, distress, discomfort, or resistance during patching or atropine administration, difficulty fitting treatment into daily routines, or uncertainty about whether the treatment is working.
This is not simply “non-compliance.” It is often failure to activate the family. Activation means structured support that helps parents and caregivers understand the diagnosis, believe the treatment is necessary, manage practical barriers, encourage the child, respond to setbacks, and continue treatment long enough to achieve benefit. Amblyopia treatment extends far beyond the prescription. It is a behavioural and family-support process. [27]
Failure Point 7: Failure to Follow Up and Protect Gains
The final failure occurs when the child is lost after treatment begins. Vision may improve initially, but follow-up is needed to monitor response, adjust treatment, detect recurrence, support adherence, and decide when treatment can safely be reduced or stopped. Without follow-up, the system may never know whether the child achieved meaningful visual improvement. [28]
At the system-design level, this is a registry and accountability failure. If no system tracks who has started treatment, who has missed review, whose vision has improved, and who remains at risk, then no one is truly responsible for the outcome. The pathway ends not when a test is performed, but when the child’s visual function is improved, stabilised, or protected. Stabilised means that visual gains are maintained and further deterioration is avoided.
From Failure Chain to Accountability Chain
| Failure point | Typical system-design cause | Accountability response | Linked pathway stage |
| Failure to screen | Screening depends on chance detection or parental awareness rather than routine child-health platforms. | Embed screening in preschool, school, primary care, or community systems. | Identify |
| Failure to communicate risk | Families are informed, but not activated; urgency and next steps remain unclear. | Use clear communication, counselling, and understandable referral messaging. | Identify → Confirm |
| Failure to refer and navigate | Referral depends on the family alone, without reminders, appointments, or navigation support. | Create active referral tracking, reminders, and clear service destinations. | Confirm |
| Failure to confirm diagnosis | Diagnostic capacity is limited, delayed, or poorly linked to screening. | Provide timely paediatric assessment, refraction, and escalation pathways. | Confirm |
| Failure to correct | Treatment is recommended, but spectacles or specialist care are not reliably delivered. | Treat spectacles and corrective intervention as essential programme infrastructure. | Correct |
| Failure to activate treatment | Families receive a prescription but little support for daily treatment realities. | Build family activation, adherence support, and school/community reinforcement into care. | Activate |
| Failure to follow up and protect gains | No registry, review system, or outcome accountability is in place after treatment starts. | Track follow-up, monitor recurrence, and measure protected functional vision. | Protect |
The Public Health Failure Chain should not be used to blame families, teachers, clinicians, or individual programme staff. Its purpose is to reveal where the system design is incomplete. Each failure point can be redesigned as an accountability point.
This mapping shows how the Public Health Failure Chain and the Amblyopia Prevention Pathway Framework work together. The Failure Chain diagnoses where children are lost. The Pathway Framework defines what the system must deliver: Identify, Confirm, Correct, Activate, Protect.
This is the practical meaning of pathway accountability. Amblyopia prevention is not achieved by detecting risk once; it is achieved by managing the child across the full journey from identification to protected vision.
Executive Insight
Screening is not prevention unless the child receives confirmation, treatment, adherence support, and follow-up.
Part VI. Treatment and Recovery: From Prescription to Protected Vision
Amblyopia treatment is often clinically straightforward in principle, but difficult to complete in practice. The child may need spectacles, patching, atropine penalisation, treatment of strabismus, surgery for cataract or ptosis, or another intervention depending on the underlying mechanism. Yet the public-health challenge is not simply choosing the correct treatment. It is ensuring that treatment is understood, started, sustained, adjusted, and followed until visual function is improved or protected.
The clinical aim of amblyopia treatment is to improve visual function in the weaker eye, support binocular development where possible, reduce the risk of lifelong visual impairment in the amblyopic eye, and reduce future disability risk if the better-seeing eye is later injured or diseased. The pathway aim is broader: to ensure that every child who is identified and confirmed receives the intervention they need, in a form the family can access, understand, and continue. [3]
Optical Correction: The Foundation of Treatment
For many children, the first and most important treatment step is accurate refractive correction. Spectacles can improve vision substantially in children with refractive, anisometropic, strabismic, or combined amblyopia, and in some cases refractive correction alone may produce significant improvement before additional therapy is required. The AAO Preferred Practice Pattern notes that treatment of refractive error alone can improve visual acuity in children with anisometropic, strabismic, combined, or bilateral refractive amblyopia. [3]
This makes spectacle access a clinical necessity, not a cosmetic or optional intervention. If a child receives a prescription but cannot obtain glasses, does not like wearing them, breaks them, loses them, or is teased for wearing them, the treatment pathway has already weakened. A health system cannot claim to treat refractive amblyopia unless it also solves the practical problem of spectacle delivery, replacement, acceptance, and continued wear.
In programme terms, optical correction should be measured as more than “prescription issued.” Useful indicators include whether spectacles were dispensed, whether they were affordable, whether the frame was acceptable to the child, whether the prescription was accurate, whether the child wears them consistently, and whether follow-up confirms visual improvement or residual amblyopia requiring additional treatment. Frame acceptability matters because comfort, fit, appearance, and peer acceptance affect willingness to wear spectacles and therefore treatment effectiveness. Prescription accuracy also matters, especially in children with significant hyperopia, astigmatism, or anisometropia; cycloplegic refraction should be used where indicated and available. [16]
Patching and Atropine: Effective but Behaviourally Demanding
If visual improvement with spectacles alone is insufficient, occlusion therapy with patching or pharmacological penalisation with atropine may be recommended. Patching works by covering the better-seeing eye so that the brain is encouraged to use the amblyopic eye. Atropine penalisation blurs vision in the stronger eye, usually for near tasks, encouraging use of the weaker eye. Treatment choice depends on the child’s age, amblyopia severity, clinical mechanism, family circumstances, and specialist assessment.
The evidence base supports both patching and atropine as effective treatments for many children. Landmark Pediatric Eye Disease Investigator Group studies and Cochrane-level evidence have contributed to modern treatment approaches, including shorter patching regimens for selected cases of moderate amblyopia and the use of atropine as an alternative in appropriate children. However, treatment should be individualised and monitored rather than reduced to a fixed formula. [29,30,31]
These treatments are family routines as much as medical prescriptions. A patch may be uncomfortable, socially visible, or resisted by the child. It may attract questions, staring, or teasing from peers. Atropine may worry parents because it changes pupil size and blurs the stronger eye. Families may stop treatment early if they do not understand the purpose, do not see rapid improvement, or feel overwhelmed by conflict and daily effort. Treatment success therefore depends heavily on family activation, not merely clinical instruction. [27]
Treatment of the Underlying Cause
Some children need treatment beyond spectacles, patching, or atropine. Strabismus may require careful assessment, optical correction, amblyopia therapy, and sometimes surgery. Deprivation causes such as congenital cataract, severe ptosis, or media opacity may require urgent specialist intervention, followed by optical correction and amblyopia treatment. The order and timing of interventions depend on the mechanism, age, severity, and clinical context. [16,17]
This is where the distinction between screening and diagnosis becomes essential. A screening programme may identify reduced vision, abnormal red reflex, refractive risk, or ocular misalignment, but only clinical assessment can determine the underlying cause and the appropriate treatment sequence. A child with refractive amblyopia, strabismic amblyopia, deprivation amblyopia, or mixed-mechanism amblyopia should not be managed through a one-size-fits-all protocol.
From a system perspective, treatment of the underlying cause requires rapid escalation pathways. A suspected cataract or severe ptosis cannot be managed through the same routine pathway as mild refractive error. A mature amblyopia programme should therefore include urgency categories — such as urgent, semi-urgent, and routine — specialist referral routes with defined waiting-time targets, and clear communication with families about why the pathway differs from child to child.
Activation: Turning Advice Into Action
The most fragile part of amblyopia treatment is often not the prescription; it is the daily execution of the plan. Families may understand that treatment is recommended but still struggle to carry it out. They may face practical barriers, emotional resistance from the child, uncertainty about progress, embarrassment around patching or glasses, or competing pressures at home, school, and work.
The article therefore uses the term Activate deliberately. Activation is more than telling parents what to do. It means helping families understand why treatment matters, what improvement may look like, how long treatment may take, how to respond when the child resists, when to return for review, and how to seek help if the plan becomes difficult.
A programme that supports activation may include clear written instructions, parent counselling, school reinforcement, reminder systems, child-friendly patching strategies, peer-sensitive spectacle options, follow-up calls, text reminders, community health worker contact, or digital adherence support. Peer-sensitive spectacle options mean frames that children find comfortable, attractive, and socially acceptable, reducing refusal and teasing. The exact model will vary by setting, but the principle is universal: treatment plans must be designed around real family life, not idealised compliance.
Follow-Up, Adjustment, and Recurrence Prevention
Amblyopia care does not end when treatment begins. Follow-up is required to assess visual response, adjust treatment intensity, monitor the better-seeing eye, identify side effects or practical barriers, and decide when treatment should continue, change, taper, or stop. Improvement may be gradual, and some children require months or years of supervised care depending on age, severity, mechanism, and response.
Follow-up also matters because visual gains may need protection. A child whose vision improves can still be at risk of recurrence or incomplete recovery if treatment is stopped abruptly, follow-up is missed, glasses are not worn, or the underlying risk remains. Continued monitoring is therefore necessary after treatment, especially where amblyopia is associated with persistent anisometropia, strabismus, or other ongoing risk factors. [28]
At system level, follow-up should be treated as an outcome-protection function. Programmes should record more than whether treatment was prescribed. They should also record whether the child returned, whether vision improved, whether treatment was adjusted, whether recurrence risk was reviewed, and whether the final visual outcome was protected. Recurrence-risk review means assessing whether the underlying cause remains active, whether spectacles are still needed, whether alignment or refractive risk persists, and whether ongoing monitoring is required.
Newer and Digital Treatment Approaches
In recent years, binocular therapies, dichoptic treatments, virtual-reality approaches, eye-tracking systems, and digital therapeutics have attracted increasing attention. These approaches are based on the idea that amblyopia involves more than one weak eye; it also reflects disordered binocular visual processing. Some interventions aim to rebalance input between the two eyes and stimulate binocular cooperation.
These developments are promising, but they should be discussed with caution. Recent evidence has not consistently shown that binocular digital treatments outperform standard patching in the short term. Emerging digital and binocular tools may become useful parts of future care, but they require robust evidence, long-term follow-up, usability testing, equity assessment, and integration into clinical pathways. [32]
For public-health programmes, the lesson is clear: innovation should be welcomed, but not allowed to distract from the fundamentals. The highest-value treatment system is one that reliably delivers accurate diagnosis, spectacles, patching or atropine where indicated, family support, follow-up, and outcome monitoring. New technologies should strengthen that pathway, not replace it.
Measuring Treatment Success
Treatment success should not be measured only by whether a therapy was prescribed. A child-centred and system-centred approach should measure whether the child obtained the intervention, used it, tolerated it, returned for review, improved in vision, maintained gains, and was protected from further avoidable loss.
Practical indicators, aligned with the Amblyopia Prevention Pathway Framework, include:
- Correct: proportion of diagnosed children receiving spectacles, treatment, or specialist intervention; time from screening failure to clinical assessment; time from prescription to spectacle delivery; accuracy and appropriateness of refractive correction.
- Activate: proportion of children wearing spectacles at follow-up; proportion starting patching, atropine, or other therapy where indicated; adherence-support contacts completed; family understanding and confidence in continuing treatment.
- Protect: visual acuity improvement in the amblyopic eye; recurrence or deterioration after treatment reduction; follow-up completion rate; final protected functional vision.
Final protected functional vision means that vision in the amblyopic eye is improved or maintained at a level that supports the child’s functional development, protects the gains achieved through treatment, and reduces future disability risk if the fellow eye is later injured or diseased.
These indicators shift amblyopia treatment from an individual prescription model to a pathway-outcome model. The aim is to move beyond treating the eye and protect the child’s visual development through a system that can deliver treatment reliably.
Executive Insight
Amblyopia treatment begins with a prescription but succeeds as a family-supported pathway from correction to protected vision.
Part VII. AI, Digital Screening, and Governed Innovation
Digital tools and artificial intelligence are increasingly discussed as ways to strengthen childhood vision screening. In amblyopia prevention, their greatest value lies less in replacing clinicians than in helping health systems find children earlier, standardise risk detection, support referral triage, reduce missed cases, and track whether children move through the pathway from screening to protected vision. [6,8,19,33,34,35]
The most important distinction is this: AI and digital tools usually detect amblyopia risk factors; they do not, by themselves, diagnose amblyopia. Amblyopia remains a clinical diagnosis that requires appropriate assessment, including visual acuity, cycloplegic refraction where indicated, ocular alignment, ocular health, age, mechanism, and visual development. A tool may identify refractive risk, anisometropia, strabismus, abnormal red reflex, ptosis, or reduced visual performance, but the child still requires clinical confirmation and pathway-based care. [3,16]
This distinction protects children, families, clinicians, and health systems from two opposite errors. The first error is techno-utopianism: assuming that an app, device, algorithm, or camera-based platform can solve amblyopia prevention alone. The second error is techno-scepticism: rejecting digital tools because they are imperfect. The more mature position is governed innovation — using technology where it strengthens the pathway, while maintaining clinical accountability, equity, and outcome monitoring.
What Digital Tools Can Add
Digital tools can support amblyopia prevention in several ways. Instrument-based screening and photoscreening may help identify refractive risk factors and ocular alignment concerns, especially in young children who cannot reliably complete standard visual-acuity testing. Smartphone-based vision-screening and referral platforms may help screen children in schools, communities, and primary-care settings. Digital referral systems may help track failed screening results, appointment attendance, treatment initiation, follow-up, and outcomes. [14,34,35]
Evidence from smartphone-supported eye-health programmes speaks directly to the challenges of low- and middle-income settings. The Peek school eye-health trial in Kenya showed that a smartphone-based school screening and referral system could improve identification and referral processes compared with standard approaches, including improved follow-up attendance in the intervention pathway. These studies make an important point: the value of digital health lies in connecting detection to referral and service use, not simply in testing vision. [8]
Recent reviews also suggest growing interest in smartphone applications and AI-supported paediatric eye screening, including tools for visual acuity testing, refractive risk detection, strabismus screening, and broader paediatric eye-disease detection. However, the evidence base remains heterogeneous, with variation in study design, population, device type, outcome definitions, and clinical validation. This supports cautious implementation rather than premature generalisation. [34,35]
AI and Strabismus Detection
AI may be particularly useful in areas where visual signs can be captured by images, video, or eye-tracking data. Strabismus detection is one such area. Recent systematic-review evidence suggests promising performance of AI models in strabismus screening, while also emphasising the need for diverse populations, multimodal data, and further work before clinical utility can be fully established. [33]
This matters for amblyopia because strabismus is a major amblyopia risk factor. If AI-supported tools can help detect suspected strabismus earlier in community or school settings, they may support earlier referral. However, suspected strabismus detected by an algorithm should not be treated as a final diagnosis. The child still needs clinical assessment, ocular alignment evaluation, refractive assessment, and amblyopia-risk evaluation.
Digital Referral and Tracking May Matter More Than the Algorithm
In many programmes, the largest loss does not occur at the moment of screening. It occurs after screening, when the child fails to attend assessment, does not receive spectacles, does not start treatment, or is lost to follow-up. Digital referral and tracking systems may therefore be as important as screening algorithms.
A strong digital amblyopia programme should be able to answer practical questions: Which children were screened? Who failed? Who was referred? Did the family receive the result? Was an appointment made? Did the child attend? Was a diagnosis confirmed? Were spectacles dispensed? Was patching, atropine, or other treatment started? Did follow-up occur? Did vision improve or remain protected?
This is where digital systems can transform programme management. A paper referral slip may disappear. A registry can identify children who have not attended. A text message can remind families. A dashboard can show where children are being lost. A programme manager can compare schools, districts, clinics, or outreach teams. Used well, digital health can convert invisible pathway failure into measurable system intelligence.
Governance Requirements for AI and Digital Screening
AI in children’s eye care should be governed carefully because the stakes include children’s health, family trust, clinical safety, data protection, and equity. WHO’s guidance on ethics and governance of AI for health emphasises principles such as protecting autonomy, promoting human well-being and safety, ensuring transparency and explainability, fostering responsibility and accountability, ensuring inclusiveness and equity, and promoting responsive and sustainable AI. [6]
For amblyopia screening, these principles translate into practical requirements:
- Clinical validity: The tool must detect relevant amblyopia risk factors accurately in the target age group.
- Population validation: The tool should be tested in the populations where it will be used, including diverse ethnic groups, languages, skin tones, facial features, children with developmental delay or neurodevelopmental conditions, socioeconomic settings, and resource contexts.
- Clinical confirmation: Positive screening results must lead to appropriate eye examination, not automated diagnosis.
- Equity safeguards: Implementation should reduce disparities in access to eye care, not widen them by serving only digitally connected or well-resourced communities.
- Data protection: Children’s images, vision results, referral records, and health information must be collected, stored, and shared securely, with appropriate consent from parents or guardians and, where possible, assent from the child.
- Workflow integration: The tool must fit into real clinical, school, and community workflows, rather than generating referrals that overwhelm services or data demands that burden staff.
- Accountability: A responsible person, clinic, school-health team, or programme office must own the next step after a failed screen. Accountability should be assigned to a named role or team, not left to diffuse system responsibility.
- Outcome monitoring: The programme must measure referral completion, treatment initiation, follow-up, and visual outcomes rather than screening volume alone.
The Risk of Digital Inequity
Digital tools are sometimes presented as solutions for low-resource settings, but they can also introduce new forms of inequity. A device may require reliable electricity, internet connectivity, maintenance, software updates, subscription fees, compatible phones, trained personnel, language adaptation, or cloud infrastructure. A system may work well in a pilot project but fail when scaled into rural schools, remote communities, or underfunded primary-care networks. [6,13]
The opposite risk also exists: high-income systems may have advanced screening devices but still fail because referral tracking, family communication, spectacle access, and follow-up remain weak. Technology does not automatically create accountability. A well-funded system can still lose children after screening if no one is responsible for pathway completion.
Equity-focused digital design therefore requires asking two questions together: “Does the tool work?” and “For whom does it work, where does it work, who is missed, who pays, who follows up, and what happens after a positive result?”
AI Must Support, Not Replace, Human Accountability
The role of AI in amblyopia prevention should be framed as pathway support. AI may help identify children who need further assessment. It may help standardise screening, prioritise referral, detect patterns, monitor programme gaps, or support health education. But AI cannot counsel a parent, examine a child comprehensively, prescribe treatment responsibly, judge family barriers, manage distress during patching, or ensure that follow-up occurs.
AI governance in amblyopia prevention must therefore be connected to the broader care pathway. A technically impressive algorithm that does not improve referral completion or visual outcomes falls short as a public-health tool. Algorithmic accuracy alone is not the outcome that matters. What counts is whether more children are confirmed, corrected, activated, followed up, and protected.
Digital Innovation in Low-Resource Settings
In low- and middle-income settings, the most valuable digital solution may be simple, robust, and pathway-oriented rather than technologically complex. A mobile platform that records failed screening, sends referral reminders, tracks attendance, links to affordable spectacles, and alerts community workers when a child is lost may have greater population impact than an advanced AI system that cannot be maintained or scaled.
This does not mean low-resource settings should receive inferior technology. It means technology must match local infrastructure, workforce, cost structure, language, culture, and service capacity. Programmes should be designed around sustainability: training, maintenance, supervision, referral capacity, data governance, and long-term financing.
A Practical Governance Checklist
Before adopting an AI or digital tool for amblyopia-related screening, programme leaders should ask:
Problem and purpose
- What exact problem is the tool solving: detection, referral, tracking, triage, counselling, adherence, or monitoring?
- Does it detect amblyopia directly, or does it detect amblyopia risk factors?
Clinical validity
- Has it been validated in the target age group and population?
Pathway and accountability
- What happens after a positive result? Is there a defined, resourced, and accountable referral pathway that ensures clinical assessment?
- Who confirms the diagnosis?
- Who explains the result to the family?
Ethics and data
- How are privacy, consent, image storage, and data sharing managed?
Infrastructure and cost
- Does the tool work offline or in low-connectivity environments if needed?
- What are the costs of devices, licences, maintenance, training, and replacement?
Equity and outcomes
- Could the tool widen inequity by excluding children without digital access?
- What indicators will show that the tool improves referral completion, treatment access, follow-up, and visual outcomes—the measures that matter within the Amblyopia Prevention Pathway Framework?
If these questions cannot be answered, the programme is not ready for responsible digital implementation.
Executive Insight
AI can help detect amblyopia risk factors and support triage, but it cannot replace clinical confirmation, governed referral pathways, or human accountability.
Part VIII. The Amblyopia Prevention Pathway Framework: Identify, Confirm, Correct, Activate, Protect
The preceding sections show that amblyopia prevention cannot be reduced to a screening event, a spectacle prescription, or a patching regimen. It requires a complete pathway that links early detection to confirmed diagnosis, appropriate correction, family-supported treatment, follow-up, and measurable visual outcomes. The Amblyopia Prevention Pathway Framework is proposed as a practical model for designing, monitoring, and improving childhood vision services. [3,4,5]
The framework has five stages: Identify, Confirm, Correct, Activate, Protect. Each stage represents a necessary function in preventing avoidable visual impairment from amblyopia. Each stage is necessary, but insufficient alone. A child can be identified but not confirmed, confirmed but not corrected, corrected but not activated, activated but not protected through follow-up. Prevention therefore depends on pathway completion, not isolated activity.
| Framework stage | Strategic purpose | What the system must deliver | Desired programme result |
| Identify | Find children at risk early. | Age-appropriate screening, outreach, and inclusive case finding. | Children at risk are recognised before avoidable visual loss becomes entrenched. |
| Confirm | Establish diagnosis and mechanism. | Clinical assessment, refraction, ocular alignment, and ocular health evaluation. | Screen-positive children receive timely diagnostic confirmation and triage. |
| Correct | Translate diagnosis into treatment action. | Spectacles, specialist treatment, and correction of underlying causes. | Recommended treatment is actually received, not merely prescribed. |
| Activate | Convert clinical advice into sustained family action. | Counselling, adherence support, school reinforcement, reminders, and practical help. | Families understand treatment and are supported to continue it. |
| Protect | Maintain gains and secure long-term outcome. | Follow-up, response monitoring, recurrence prevention, and discharge planning. | Visual gains are sustained and functional vision is protected over time. |
Stage 1: Identify
The first responsibility of the system is to identify children who may have amblyopia or amblyopia risk factors. Identification may occur through preschool screening, school-based screening, child-health checks, primary-care visits, community outreach, red-reflex assessment, visual-acuity testing, photoscreening, autorefraction, instrument-based screening, or referral triggered by parental or teacher concern. [4,14,16,17]
The purpose of Identify is not to label a child with amblyopia. It is to detect risk early enough to justify further assessment. This distinction is important because screening is not diagnosis. A failed screen should trigger a pathway, not create false certainty or false reassurance.
Useful indicators for the Identify stage include population coverage, screening uptake, age at screening, proportion failing screening, proportion referred, and whether screening reaches vulnerable groups. A mature programme should be able to answer how many children were screened, which children were missed, which schools or communities were under-covered, and whether high-risk children were reached, including those with family history of amblyopia or strabismus, developmental delay, neurodevelopmental conditions, known ocular risk factors, or reduced access to routine eye care.
Stage 2: Confirm
The second responsibility is to confirm the diagnosis and mechanism. Amblyopia cannot be managed properly unless the underlying cause is understood. A child may have refractive amblyopia, strabismic amblyopia, deprivation amblyopia, mixed-mechanism amblyopia, or another eye condition requiring a different response.
Confirmation requires appropriate clinical assessment, which may include age-appropriate visual-acuity testing, cycloplegic refraction where indicated, ocular alignment assessment, ocular health examination, binocular vision assessment where feasible, and evaluation for deprivation causes such as cataract or ptosis. The exact assessment model will vary by setting, but the principle is universal: a screening result must be connected to competent clinical confirmation. [16]
Useful indicators for the Confirm stage include time from failed screening to examination, attendance rate after referral, diagnostic confirmation rate, proportion requiring spectacles, proportion requiring specialist referral, and proportion requiring urgent escalation. Urgent escalation may include suspected cataract, severe ptosis, media opacity, abnormal red reflex, or other findings requiring rapid specialist assessment. A programme that identifies many children but cannot confirm diagnosis in a timely way has created demand without delivering care.
Stage 3: Correct
The third responsibility is to correct the optical, anatomical, or functional problem that is driving amblyopia risk. For many children, this begins with accurate spectacles. For others, correction may require treatment of strabismus, cataract, ptosis, media opacity, or another underlying condition. Correction is therefore not a single intervention; it is the stage at which diagnosis is translated into action.
Spectacle correction warrants special attention. In refractive and anisometropic amblyopia, spectacles are often the foundation of treatment. Yet many programmes still treat spectacle provision as a minor logistical issue rather than a core clinical function. This is a mistake. A prescription that does not become a pair of accurate, affordable, acceptable, and consistently worn spectacles is not a completed intervention. [3,20]
Correction should be measured by whether the child actually receives the intervention, not by whether it was recommended. Useful indicators include spectacle dispensing rate, time from prescription to spectacle delivery, affordability, frame acceptability, replacement access, treatment initiation rate, urgent referral completion, and clinical response to initial correction. Clinical response to initial correction includes improvement in visual acuity with spectacles alone, which may reduce or occasionally eliminate the need for additional amblyopia therapy, while also identifying children who require patching, atropine, or further specialist treatment.
Executive Insight
Spectacle access is not a minor logistical issue; it is a public-health supply-chain requirement for preventing avoidable childhood visual impairment.
Stage 4: Activate
The fourth responsibility is to activate the family and care environment. Activation means converting clinical advice into sustained action. It recognises that amblyopia treatment happens in homes, classrooms, daily routines, and family relationships as much as in clinics.
A child may resist spectacles, remove a patch, struggle with atropine, feel embarrassed, or become frustrated by treatment. Parents may understand the recommendation but still face cost, transport, time pressure, worry, stigma, or treatment fatigue. Teachers may not know that the child needs support. Community workers may not know who has been lost after referral. Without activation, even correct clinical advice may fail. [27]
Activation requires structured communication, practical support, and behavioural follow-through. This may include parent counselling, clear written instructions, reminder systems, school reinforcement, community health worker contact, child-friendly patching strategies, peer-sensitive spectacle options, and digital adherence support. The aim is not to blame families for non-adherence; it is to design care around the realities families face.
Useful indicators for the Activate stage include treatment-start rate, spectacle-wear rate at follow-up, patching or atropine adherence, parent understanding, school support, follow-up contact completion, and documented response when a family struggles to continue treatment. This documented response should trigger escalation of support, not simply record non-adherence.
Stage 5: Protect
The fifth responsibility is to protect visual gains. Amblyopia care does not end when treatment begins or when vision first improves. Children may need ongoing monitoring, treatment adjustment, recurrence prevention, spectacle updates, assessment of binocular function, and support during treatment tapering or discontinuation. [28]
Protect is the stage that converts short-term improvement into long-term outcome. It asks whether the child’s visual development has been stabilised, whether the amblyopic eye has improved or maintained useful function, whether the better-seeing eye is protected by reducing dependence on one eye alone, and whether the system knows the final outcome.
Useful indicators for the Protect stage include follow-up completion rate, visual acuity improvement, stability of gains, recurrence or deterioration after treatment reduction, ongoing spectacle use, final protected functional vision, and documented discharge or long-term monitoring plan. Final protected functional vision means visual acuity that is improved or maintained at a level supporting the child’s functional development, preserving treatment gains, supporting binocular function where possible, and reducing future disability risk if the fellow eye is later injured or diseased.
The Framework as a Management Tool
| User / decision-maker | How the framework is used | Primary management value |
| Clinicians | Connect diagnosis, treatment, adherence support, and follow-up as one continuum of care. | Prevents clinical care from stopping at prescription alone. |
| Schools / school-health teams | Recognise that screening is only the first step and support communication, referral, and follow-up. | Turns schools from testing sites into pathway partners. |
| Public-health planners | Define indicators and monitor pathway completion across populations and settings. | Moves programmes from activity reporting to measurable prevention. |
| Healthcare executives / programme managers | Build dashboards, identify drop-off points, and target quality-improvement action. | Shows exactly where children are being lost and who must respond. |
| Policymakers / system leaders | Assign accountability across sectors, set standards, and align financing and governance. | Creates shared ownership for child-vision outcomes. |
Part IX. Implementation Roadmap: From Framework to Measurable Change
Amblyopia prevention requires more than agreement with the principle of early screening. It requires implementation discipline. Health systems must decide who will be screened, where screening will occur, how referrals will be managed, who will confirm diagnosis, how spectacles and treatment will be delivered, how families will be supported, and how outcomes will be measured. [5,9,13]
The Amblyopia Prevention Pathway Framework provides the structure, but implementation requires staged action. A practical roadmap should begin with achievable steps, build toward integrated pathways, and ultimately create a mature child-vision system that can identify, confirm, correct, activate, and protect children at scale.
This roadmap is presented across three time horizons: 100 days, 1 year, and 5 years. The purpose is not to prescribe one universal model, but to demonstrate a staged approach by which any programme — regardless of starting point — can move from fragmented activity toward accountable prevention.
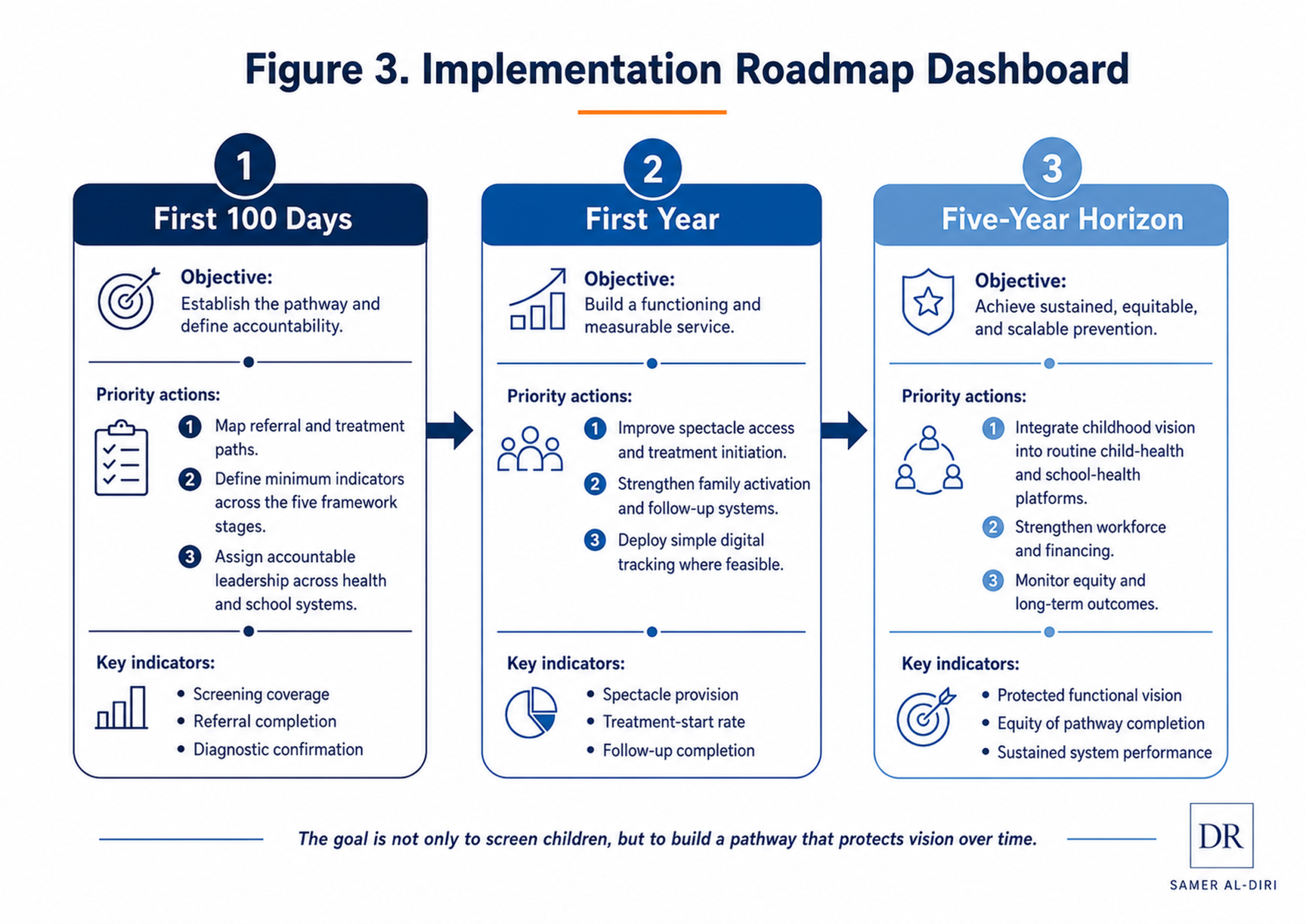
Figure 3. Implementation Roadmap Dashboard. A staged 100-day, first-year, and five-year approach for turning amblyopia prevention into measurable system performance.
The First 100 Days: Build the Pathway Foundation
The first 100 days should focus on mapping the current system, identifying bottlenecks, and creating a minimum viable pathway. The goal is not to build a perfect national programme immediately. The goal is to stop treating screening, referral, spectacle access, treatment, and follow-up as disconnected activities.
A practical first step is to conduct a pathway audit. A small multi-stakeholder team — including school-health, eye-care, public-health, and administrative representatives — should conduct this audit together. Programme leaders should map what happens to a child from the moment of screening to the final visual outcome. This audit should ask: Where are children screened? Who performs screening? What happens after a failed result? How is the family informed? Where is the child referred? How long does assessment take? Are spectacles affordable and available? Who follows up? Where are outcomes recorded? [5,13]
The first 100 days should also define minimum indicators across the five framework stages:
| Framework stage | Minimum early indicators | Immediate management question |
| Identify | Children eligible, screened, failed screening, and referred. | Are children at risk being found, and are key groups being missed? |
| Confirm | Children attending clinical assessment and receiving diagnosis. | Does referral lead to timely diagnostic confirmation? |
| Correct | Children receiving spectacles, treatment, or specialist intervention. | Are recommended interventions actually reaching children? |
| Activate | Children starting treatment and receiving family support. | Are families being helped to begin and sustain care? |
| Protect | Children returning for follow-up and showing improved or protected vision. | Is the programme measuring maintained benefit rather than initial activity alone? |
At this early stage, the programme does not need a sophisticated digital platform to begin. A spreadsheet, simple registry, paper logbook, or school-health register may be enough if it captures the pathway consistently. The critical change is accountability: every failed screen should have a documented next step, and every child referred should be traceable until assessment is completed.
The first 100 days should also identify quick operational fixes. These may include standard referral forms, clearer parent communication, designated school-health contacts, agreed referral destinations, simple reminder systems, basic spectacle-provision arrangements, and defined urgency criteria for children with suspected cataract, severe ptosis, abnormal red reflex, or other high-risk findings. Urgency criteria should include a clearly defined rapid-referral route and a maximum acceptable waiting time for children who require specialist assessment.
The most important product of the first 100 days is a functioning pathway map with named responsibilities at each stage. Without this, screening remains an event. With it, screening begins to become prevention.
The First Year: Build an Integrated Programme
The first year should move the programme from pathway mapping to structured implementation. This means creating protocols, training personnel, standardising referral processes, strengthening spectacle access, and introducing systematic follow-up.
A first-year programme should define age groups and screening settings clearly. Depending on local context, screening may occur through preschool services, school-entry checks, school-health programmes, primary-care visits, community outreach, or a combination of these. The chosen model should reflect local workforce, geography, school attendance, health-system capacity, and available technology.
Training should be practical and role-specific. Teachers, nurses, community health workers, primary-care staff, optometrists, orthoptists, and ophthalmology teams do not all need the same training. Screeners need to understand how to perform age-appropriate tests and communicate results. Referral coordinators need to track attendance, communicate clearly with families, support family activation, and help families navigate the pathway. Clinical teams need capacity for paediatric refraction, ocular alignment assessment, and amblyopia management. Programme managers need dashboards that show where children are being lost.
The first year should also strengthen spectacle access as a core programme function. This may require negotiated low-cost spectacle packages, local production where feasible, regional supply-chain arrangements, school-based spectacle delivery, frame choices acceptable to children, repair and replacement mechanisms, and subsidy pathways for families who cannot afford care. Spectacle provision should be treated as a public-health supply-chain requirement, not an optional add-on. [13,20]
Family activation should also become a formal part of the programme. Parent counselling, clear written instructions, reminder messages, school reinforcement, follow-up calls, and community health worker contact can all help convert treatment advice into daily action. The programme should not wait until families are labelled “non-adherent” before offering support. Activation should be proactive, universal, and built into the pathway from the first point of contact.
By the end of the first year, a mature early programme should be able to report more than screening coverage. It should report referral completion, diagnostic confirmation, spectacle delivery, treatment initiation, follow-up attendance, and visual outcome indicators. The first-year objective is to shift from activity reporting to pathway reporting.
The Five-Year Horizon: Build a Mature Childhood Vision System
The five-year goal is a mature, integrated childhood vision system embedded within public health, education, primary care, eye-care services, and health information systems. At this stage, amblyopia prevention should no longer depend on isolated campaigns, individual champions, or short-term projects. It should become a routine function of child-health systems.
A mature five-year system should include stable governance. This means clear ownership across ministries of health, ministries of education, school-health authorities, eye-care providers, public-health departments, and financing bodies. Each organisation should understand its role in the pathway. Schools may support identification and communication. Primary care may support early detection and referral. Eye-care services may confirm diagnosis and manage treatment. Public-health teams may monitor indicators. Policymakers may ensure financing, standards, and accountability.
The five-year horizon should also include integrated data systems. These do not need to be complex, but they should allow programmes to track children across the pathway. A mature system should know which children were screened, which children failed, which children attended assessment, which received spectacles or treatment, which returned for follow-up, and which achieved improved or protected vision. Data should serve quality improvement, not reporting alone.
Digital tools and AI may have a role in the five-year system, but only where they strengthen the pathway. Instrument-based screening, smartphone referral platforms, registries, reminder systems, adherence tools, and dashboards may all be useful if validated, governed, equitable, and integrated. The measure of success should not be whether the system has advanced technology, but whether the technology helps more children complete the pathway. [6,8]
A mature childhood vision system should also include continuous quality improvement. Programmes should establish a regular review cycle, such as quarterly or twice-yearly review, to examine pathway data, identify drop-off points, and implement targeted improvements. Programmes should regularly review false-positive and false-negative concerns, referral delays, spectacle delivery times, family barriers, treatment adherence, recurrence, and outcomes. Improvement should be targeted where the largest drop-offs occur. If many children are screened but few attend assessment, referral navigation is the priority. If many are diagnosed but few receive spectacles, supply-chain and financing are the priority. If many start treatment but few complete follow-up, activation and tracking are the priority.
The five-year ambition extends beyond reducing amblyopia-related visual impairment. It aims to create a child-vision system capable of detecting preventable eye problems early, connecting families to care, supporting treatment, and protecting long-term visual development.
Resource-Adapted Implementation Tiers
Amblyopia prevention should be adapted to available resources without abandoning core pathway principles. Every setting, whether highly resourced or severely constrained, should still aim to identify, confirm, correct, activate, and protect.
In minimal-resource settings, the priority may be basic school or community visual-acuity screening, red-reflex awareness, simple referral registers, clear parent communication, affordable spectacle pathways, and community follow-up. The programme may rely on teachers, nurses, or community health workers for initial identification and referral support, with clinical confirmation provided through periodic outreach or referral to regional services.
In intermediate-resource settings, programmes may add preschool screening, trained school-health teams, optometry or orthoptic involvement, structured spectacle delivery, defined referral targets, mobile data collection, and regular programme dashboards. These systems should prioritise referral completion and spectacle access, because these are common points of loss.
In higher-resource settings, programmes may include instrument-based screening, digital registries, integrated electronic referral, automated reminders, AI-supported risk triage, paediatric ophthalmology networks, and advanced outcome dashboards. However, higher-resource systems should not assume that technology alone guarantees success. They must still measure pathway completion and visual outcomes.
The principle is simple: resources may change the tools, but they should not change the accountability pathway.
Leadership and Governance
Implementation requires leadership. Childhood vision programmes often fail because responsibility is diffuse. Schools assume families will act. Families assume clinics will manage. Clinics assume the child will return. Public-health teams count screening activity. No single actor owns the full outcome.
A mature programme should assign responsibility at each stage. There should be a named team or role responsible for screening coverage, referral tracking, diagnostic capacity, spectacle access, treatment activation, and follow-up monitoring. Accountability should not be punitive; it should be used to identify gaps, allocate resources, and improve the pathway.
Governance should also include standards for safety, equity, and data protection. Children’s health information must be handled securely. Screening tools should be validated. Referral pathways should be realistic. Families should receive understandable communication. High-risk children should not be missed because they are outside school, have developmental delay, live rurally, or face financial barriers. Programmes should actively identify and reach these children through alternative mechanisms, including community outreach, disability services, primary-care networks, financial support, and targeted follow-up.
Executive Insight
The success of an amblyopia programme should not be measured by how many children are screened, but by how many children achieve protected, functional vision.
A Practical Implementation Dashboard
| Dashboard domain | Illustrative metric | What leaders should ask | Action if performance is weak |
| Identify | Screening coverage and referral initiation | Which children, schools, or vulnerable groups are being missed? | Expand reach, standardise screening, and close coverage gaps. |
| Confirm | Referral completion and time to examination | Are failed screens leading to timely clinical assessment? | Improve referral navigation, appointment support, and diagnostic capacity. |
| Correct | Spectacle delivery and treatment initiation | Are children receiving the intervention that has been prescribed? | Strengthen spectacle access, subsidy, procurement, and clinical follow-through. |
| Activate | Treatment-start rate and family-support completion | Are families able to understand, begin, and continue treatment? | Add counselling, reminders, school reinforcement, and targeted support. |
| Protect | Follow-up completion and protected functional vision | Are gains being sustained and outcomes recorded? | Track children longitudinally, monitor recurrence, and improve review systems. |
| Equity | Performance by geography, school attendance, disability, or social vulnerability | Which groups are systematically lost from the pathway? | Target outreach, alternative delivery channels, and resource allocation. |
From Roadmap to System Transformation
The implementation roadmap turns the Amblyopia Prevention Pathway Framework into practical action. The first 100 days create the minimum pathway. The first year builds an integrated programme. The five-year horizon embeds amblyopia prevention into a mature childhood vision system.
The deeper lesson is that amblyopia prevention is not achieved through isolated campaigns or screening days alone. It is achieved through system design: clear responsibilities, measurable indicators, accessible treatment, family activation, follow-up, and continuous improvement.
Amblyopia is preventable not because every cause can be avoided before it occurs, but because many of its lifelong visual consequences can be reduced when health systems act early, reliably, and completely.
Part X. Policy and Leadership Brief: Turning Amblyopia Prevention Into System Accountability
This section may be read as a standalone policy brief for ministries, healthcare leaders, school-health systems, eye-care services, NGOs, development partners, and digital-health stakeholders.
Amblyopia prevention is a clinical responsibility, but it is also a leadership responsibility. Children are lost not because clinicians lack knowledge of amblyopia, but because systems often fail to connect screening, referral, diagnosis, spectacle access, treatment support, and follow-up into one accountable pathway.
The policy challenge is therefore clear: childhood vision programmes must move from activity-based reporting to outcome-based accountability. Screening coverage is important, but it is not enough. A successful programme should be judged by whether children at risk are identified early, clinically confirmed, corrected, supported, followed up, and protected from avoidable lifelong visual impairment.
Core Policy Position
Amblyopia should be recognised as a preventable childhood vision pathway failure when health systems detect risk but fail to complete care. Public policy should therefore treat amblyopia prevention as part of child health, early childhood development, school health, primary eye care, educational equity, and health-system strengthening. [5,9]
This requires a shift in language and measurement. Programmes should not ask only, “How many children were screened?” They should ask:
- How many children at risk were identified?
- How many received clinical confirmation?
- How many received spectacles or specialist treatment?
- How many families were activated and supported?
- How many children completed follow-up?
- How many achieved improved or protected functional vision?
These questions convert amblyopia prevention from a screening campaign into a measurable child-health pathway.
Recommendation 1: Make Childhood Vision Screening a Connected Pathway, Not a Stand-Alone Event
Ministries of health, school-health authorities, and eye-care leaders should define childhood vision screening as the first stage of a complete pathway. Every failed screen should have a documented referral destination, a responsible follow-up mechanism, and a clear route to clinical assessment. [12,13]
Screening without referral completion should be considered an incomplete intervention. Referral without diagnostic capacity should be considered an implementation gap. Diagnosis without spectacle or treatment access should be considered a pathway failure. Treatment without follow-up should be considered incomplete care.
Recommendation 2: Adopt the Amblyopia Prevention Pathway Framework
Policymakers and programme leaders should use the Amblyopia Prevention Pathway Framework — Identify, Confirm, Correct, Activate, Protect — as a practical structure for programme design, monitoring, and quality improvement.
This framework can be used to define indicators, assign responsibility, identify bottlenecks, design dashboards, and compare programme performance across schools, districts, clinics, or regions. Its value lies in its simplicity: every child should move through each stage unless clinical assessment confirms that no further action is required.
Recommendation 3: Measure Pathway Completion, Not Screening Volume Alone
Childhood vision programmes should report pathway-completion indicators. At minimum, this should include children eligible, screened, failed, referred, examined, diagnosed, treated, followed up, and achieving improved or protected visual function.
A programme that screens many children but cannot show referral completion, spectacle delivery, treatment initiation, or visual outcome improvement is not yet demonstrating prevention. Data should support active programme management, not reporting alone: identifying where children are lost, diagnosing the cause of drop-off, and directing resources to the weakest stage of the pathway.
Recommendation 4: Treat Spectacles as Essential Childhood Eye-Care Infrastructure
Spectacle provision should be treated as a core health-system function, not a secondary commodity. For many children with refractive or anisometropic amblyopia, accurate spectacles are the foundation of treatment. Without affordable, acceptable, durable, and replaceable spectacles, screening and diagnosis cannot translate into visual recovery.
Policy should therefore address financing, procurement, distribution, school-based delivery where feasible, repair and replacement, and frame acceptability for children. Spectacle access should be part of programme design from the beginning, not added later as an afterthought.
Recommendation 5: Build Family Activation Into the Pathway
Amblyopia treatment depends heavily on family understanding and daily follow-through. Policymakers and service leaders should avoid treating adherence as a private family problem after prescription. Instead, family activation should be designed into the programme.
This includes clear communication, parent counselling, reminder systems, school reinforcement, child-friendly treatment strategies, culturally appropriate education, community health worker support where available, and practical responses when families struggle. Culturally appropriate education means using relevant languages, understandable concepts, and respectful communication. It also means developing materials that recognise family beliefs, fears, and experiences of stigma, and that address the practical barriers families face around eye care, spectacles, patching, atropine, and follow-up.
The aim is not to blame families for non-adherence, but to design services around real barriers.
Recommendation 6: Use Schools as Equity Platforms, but Do Not Rely on Schools Alone
Schools are powerful platforms for reaching children who might not otherwise access eye care. They can support screening, parent communication, spectacle delivery, follow-up reminders, and educational support. School-health systems should therefore be central to amblyopia prevention. [9,13]
However, school-based programmes should not be the only mechanism. Some children are too young for school, absent from school, outside formal education, disabled, rurally located, socially marginalised, or affected by early-onset deprivation causes that require detection before school age. Childhood vision policy should connect school health with newborn checks, early-childhood health visits, primary care, community outreach, and specialist referral pathways.
Recommendation 7: Govern AI and Digital Tools as Pathway-Support Technologies
AI, photoscreening, instrument-based screening, smartphone platforms, digital registries, referral dashboards, and reminder systems may strengthen amblyopia prevention. Their role should be to support risk detection, referral triage, pathway tracking, family communication, and outcome monitoring. [6,7,33,34,35]
However, digital tools should not be treated as substitutes for clinical confirmation or human accountability. AI and digital tools usually detect amblyopia risk factors; they do not, by themselves, diagnose amblyopia. Responsible implementation requires validation, equity safeguards, data protection, consent processes, workflow integration, and named accountability for follow-up after a positive result.
Recommendation 8: Create Resource-Adapted but Accountability-Consistent Models
Different settings will require different tools, but the accountability pathway should remain constant. Minimal-resource settings may begin with teacher-supported visual-acuity screening, red-reflex awareness, simple referral logs, affordable spectacle pathways, and community follow-up. Intermediate-resource settings may add trained school-health teams, optometry or orthoptic involvement, mobile data systems, and structured spectacle delivery. Higher-resource settings may add digital registries, automated reminders, instrument-based screening, AI-supported triage, and integrated electronic referral. [13,17]
The tools may differ, but the question remains the same: is the child identified, confirmed, corrected, activated, and protected?
Recommendation 9: Assign Named Responsibility Across the Pathway
Amblyopia prevention often fails when responsibility is diffuse. Schools may assume families will act. Families may assume clinics will manage. Clinics may assume children will return. Public-health teams may count screening activity without tracking outcomes.
Leadership should assign named responsibility for each stage of the pathway. Someone must own screening coverage. Someone must own referral tracking. Someone must own diagnostic capacity. Someone must own spectacle access. Someone must own family activation. Someone must own follow-up and outcome monitoring.
Named responsibility should be documented in programme plans, reflected in job descriptions or terms of reference, and reviewed regularly as part of programme performance assessment. Accountability should not be punitive. It should be used to identify gaps, allocate resources, improve services, and prevent children from disappearing between organisations.
Recommendation 10: Integrate Amblyopia Prevention Into Child Development and Educational Equity Policy
Vision is not separate from learning, development, participation, and future opportunity. Amblyopia prevention should therefore be positioned as more than an ophthalmology issue: it is also a child-development and educational-equity intervention.
Ministries of health and education should collaborate on shared objectives: early detection, referral completion, spectacle access, classroom support, family communication, and measurable visual outcomes. Investment in childhood vision protection is an investment in human capital, learning readiness, and long-term opportunity.
Leadership Priorities by Stakeholder Group
| Stakeholder group | Leadership priority | Immediate executive actions |
| Ministry of Health / public-health leadership | Make amblyopia prevention a measurable child-health pathway, not a stand-alone screening event. | Adopt pathway indicators, assign accountability, and link screening to diagnostic and treatment capacity. |
| Ministry of Education / school-health systems | Use schools as equity platforms for detection, communication, and follow-through. | Support screening delivery, parent communication, referral reminders, and classroom support. |
| Eye-care services | Provide timely confirmation, treatment, and follow-up for children who fail screening. | Ensure paediatric assessment capacity, spectacle pathways, urgent escalation, and outcome monitoring. |
| Healthcare executives / programme managers | Run the pathway as a managed service with visible handovers and dashboards. | Track bottlenecks, review performance regularly, and direct resources to the weakest stage. |
| Digital-health / AI partners | Support the pathway rather than displace clinical accountability. | Validate tools, protect data, and prove impact on referral completion, equity, and outcomes. |
| Development partners / NGOs / funders | Invest in scalable models that strengthen systems rather than short-lived campaigns. | Support workforce training, spectacle access, data systems, and evaluation of pathway completion. |
Minimum Policy Indicators
At national, regional, or programme level, amblyopia prevention should include a minimum indicator set aligned with the Amblyopia Prevention Pathway Framework. [5,13]
Identify
- screening coverage by age, school, district, and vulnerable group;
- proportion of children failing screening;
- proportion referred after failed screening.
Confirm
- proportion attending clinical confirmation;
- time from failed screening to examination;
- proportion diagnosed with amblyopia or amblyopia risk factors.
Correct
- proportion receiving spectacles or specialist treatment;
- time from prescription to spectacle delivery.
Activate
- proportion starting patching, atropine, or other therapy where indicated;
- family activation or counselling completion.
Protect
- follow-up attendance;
- visual acuity improvement;
- recurrence or deterioration after treatment reduction;
- final protected functional vision.
Equity
- equity gaps by geography, socioeconomic status, disability, school attendance, developmental vulnerability, or other relevant markers of exclusion.
Final protected functional vision means vision that is improved, maintained, or stabilised at a level that supports the child’s functional development, protects treatment gains, and reduces future disability risk if the fellow eye is later injured or diseased.
These indicators should be used for improvement, not simply reporting. Their purpose is to show where the pathway is failing and where leadership action is required.
Final Policy Message
Amblyopia prevention is achievable when health systems act early, reliably, and completely. The clinical tools already exist. The missing element in many settings is not knowledge of amblyopia, but accountable pathway design.
The policy goal should be simple: no child should fail vision screening and then disappear from the system. No child should receive a diagnosis but not obtain spectacles or treatment. No family should be expected to sustain amblyopia care without explanation and support. No programme should claim success based only on the number of children screened.
The measure of success is protected childhood vision.
Conclusion: From Early Detection to Protected Childhood Vision
Amblyopia is often described as a common paediatric eye condition, but its deeper significance is larger than the eye clinic. It is a test of whether health systems can act early, coordinate care, support families, and protect a child’s visual development before preventable impairment becomes lifelong.
The clinical knowledge already exists. Amblyopia risk factors can be detected. Diagnosis can be confirmed. Refractive error can be corrected. Patching, atropine, and specialist interventions can improve outcomes in appropriately selected children when families are supported to sustain treatment. Visual gains can be monitored and protected. The challenge is whether systems can deliver the full pathway reliably and equitably, not whether treatment exists in principle. [1,2,3,4]
This article has argued that amblyopia should be understood as a preventable public-health and health-system pathway failure when screening does not lead to completed care. A child is not protected because a screening form was completed. A child is protected when detection is followed by confirmation, correction, family activation, follow-up, and measurable visual outcome.
The Amblyopia Prevention Pathway Framework — Identify, Confirm, Correct, Activate, Protect — provides a practical structure for this shift. It reframes amblyopia prevention from an isolated screening activity into a five-stage accountability pathway. It asks health systems to move beyond counting how many children were screened and toward measuring how many children achieved protected, functional vision.
This shift matters because the weakest point in amblyopia prevention is often not clinical knowledge, but pathway design. Children may be screened but not referred, referred but not examined, diagnosed but not provided with spectacles, treated but not supported, improved but not followed. Each gap may appear small, but together they can convert a treatable childhood condition into avoidable lifelong visual impairment.
Technology can help, but it cannot replace accountability. AI, photoscreening, instrument-based screening, smartphone platforms, registries, dashboards, and reminder systems may strengthen risk detection, referral tracking, and programme monitoring. However, they must be clinically validated, ethically governed, equitably implemented, and connected to human responsibility. The purpose of digital innovation is not to make screening look modern; it is to help more children complete the pathway to protected vision. [6,7,33,34,35]
The most equitable amblyopia programmes will not wait passively for children to arrive at eye clinics. They will use schools, nurseries, primary-care visits, child-health checks, community outreach, and digital systems to find children earlier. They will also recognise that schools alone are not enough, especially for children who are too young, out of school, disabled, rurally located, socially marginalised, or affected by early-onset deprivation causes.
The most effective programmes will treat spectacles as essential childhood eye-care infrastructure, not optional commodities. They will treat family activation as a core intervention, not an afterthought. They will treat follow-up as outcome protection, not administration. They will treat data as a tool for improvement rather than reporting alone. They will assign responsibility clearly, measure pathway completion, and redesign services when children are lost.
The call to action is therefore simple but demanding. Ministries of health, ministries of education, healthcare executives, school-health leaders, eye-care professionals, public-health planners, digital-health innovators, NGOs, and researchers should work together to make childhood vision protection a measurable system responsibility.
No child should fail vision screening and disappear.
No child should receive a diagnosis but not obtain spectacles or treatment.
No family should be expected to sustain amblyopia care without explanation and support.
No programme should claim success by counting screening activity alone.
Amblyopia prevention is achievable when systems act early, reliably, equitably, and completely. The measure of success is not the number of children screened. The measure of success is protected childhood vision.
Further Explorations of Connected Themes
This section expands the strategic reading pathway introduced near the front of the article. It is placed here to connect the article’s conclusion with a wider set of system-level themes before the formal back-matter begins.
The systemic challenges discussed in this article – preventable vision loss, health-system pathway design, family-supported care, school-health implementation, and governed technological integration – extend across multiple domains in ophthalmology, public health, and healthcare management. The following publications provide deeper analysis of connected problems that inform this article’s wider intellectual context.
1. Age-Related Macular Degeneration: Population Ageing, Health-System Impact, Artificial Intelligence, and the Future of Sustainable Vision Care – a flagship analysis of chronic retinal disease as a health-system, ageing-society, and sustainable-care challenge.
2. Diabetic Retinopathy: A Preventable Cause of Blindness, Global Burden, Health-System Impact, Artificial Intelligence, and the Future of Vision Care – a foundational reference on preventable blindness pathways, screening systems, AI-enabled detection, and vision-system resilience.
3. Healthcare AI Governance: Institutional Leadership, Workforce Readiness, and Patient-Centred Accountability as Foundations for Sustainable Healthcare Transformation – the governing framework required for safe, ethical, equitable, and accountable clinical AI integration.
4. Building Resilient Health Systems: A Healthcare Management Framework for Governance, Workforce Readiness and Digital Transformation – the management and system-design framework underpinning pathway reliability, essential service protection, and sustainable healthcare transformation.
The author, Dr. Samer Al-Diri, has developed these publications as part of a coherent body of work on preventive eye care, public health ophthalmology, responsible AI adoption, and sustainable health-system design. Where available, citation records and DOI links are accessible through the corresponding article pages.
Limitations and Unresolved Questions
This article presents a strategic public-health and health-system framework for amblyopia prevention. It is not a formal systematic review, clinical guideline, or health-economic model. Its purpose is to synthesise clinical knowledge, screening principles, implementation challenges, digital-health governance, and policy priorities into a practical framework for action. Several limitations and unresolved questions should therefore be acknowledged.
Evidence Variation Across Settings
Amblyopia prevalence, screening performance, referral completion, treatment adherence, and visual outcomes vary across countries, age groups, screening methods, diagnostic criteria, and health-system contexts. Evidence from one setting may not translate directly to another. A preschool screening model developed in a high-income urban system may not be feasible in a rural, island, displaced, or low-resource context. Similarly, school-based screening results may vary depending on school attendance, screener training, referral pathways, spectacle access, and family engagement. [5,10,13]
Accordingly, the Amblyopia Prevention Pathway Framework should be adapted to local conditions rather than applied as a rigid template. The five stages — Identify, Confirm, Correct, Activate, Protect — should remain constant, but the tools used at each stage may differ according to workforce, financing, geography, school attendance rates, culture, technology, and service capacity.
Screening Age and Screening Method
There is no single universal screening age or method that fits every system. Preschool screening is strongly supported in many settings, but some causes of amblyopia risk, especially deprivation causes such as cataract or severe ptosis, require detection before school age. At the same time, younger children may be harder to screen using standard visual-acuity methods, and evidence for different screening tools varies by age, population, and implementation context. [4,14,16,18]
Further work is needed to define the most effective, feasible, and equitable screening schedules for different health systems. This includes the role of newborn checks, red-reflex assessment, early-childhood health visits, preschool screening, school-entry screening, and repeated school-age screening. The optimal model may differ between countries and even between regions within the same country.
Measuring True Prevention
A major limitation in many childhood vision programmes is that screening activity is easier to measure than visual outcome. Programmes may report the number of children screened, but not how many were clinically confirmed, received spectacles or treatment, completed follow-up, or achieved improved or protected visual function.
This creates an evidence gap. To understand whether amblyopia prevention programmes truly work, future research and programme monitoring should measure pathway completion and outcomes, not screening volume alone. The most important unanswered question is not simply whether children can be screened, but whether screening leads to durable visual benefit and protected functional vision. [10,11]
Treatment Adherence and Family Activation
Amblyopia treatment often depends on sustained family action over time. Spectacle wear, patching, atropine use, follow-up attendance, and treatment adjustment all require understanding, motivation, trust, and practical feasibility. Yet adherence is still often measured narrowly, and family barriers are sometimes treated as private behaviour rather than system-design issues.
Further research is needed on how best to support families in different cultural, socioeconomic, and educational contexts. This includes parent counselling, school reinforcement, community health worker support, reminder systems, peer-sensitive spectacles, child-friendly patching strategies, and digital adherence tools. The key question is how health systems can convert advice into sustained, family-supported action without blaming families when barriers arise. [27]
Equity and Children at Risk of Being Missed
School-based screening can be highly valuable, but it may miss children who are too young for school, absent from school, outside formal education, displaced, disabled, rurally located, socially marginalised, or affected by early-onset deprivation causes. Children with developmental delay, neurodevelopmental conditions, communication difficulties, or complex health needs may also require adapted screening and referral approaches.
A major unresolved implementation question is how childhood vision programmes can reach children outside standard school-health pathways. Future models should examine community outreach, primary-care integration, disability services, maternal and child-health platforms, mobile eye-care teams, and targeted follow-up for children at higher risk of being missed.
Digital Tools and Artificial Intelligence
AI, photoscreening, smartphone platforms, digital referral systems, and registries may strengthen amblyopia prevention, but the evidence base remains uneven. Many technologies are evaluated in controlled or pilot settings, while fewer are assessed at scale across diverse real-world populations. Performance may vary by age, cooperation, ethnicity, facial features, image quality, device type, connectivity, training, and service integration. [6,14,33,34,35]
Further evidence is needed on whether digital tools improve pathway outcomes beyond screening accuracy. Important questions include whether they increase referral completion, reduce time to diagnosis, improve spectacle delivery, support adherence, reduce inequity, and improve final visual outcomes. AI and digital systems should be evaluated by their effect on whether more children become confirmed, corrected, activated, and protected, not by algorithmic performance alone.
Cost-Effectiveness and Financing
Amblyopia prevention is likely to be valuable from a public-health perspective, but programme design decisions require better context-specific cost and financing evidence. Costs may include screening personnel, equipment, training, referral coordination, clinical assessment, spectacles, treatment, follow-up, digital systems, supervision, and quality improvement. [13,20]
Future work should compare different implementation models: school-based screening, preschool screening, primary-care screening, community outreach, digital referral platforms, school-based spectacle delivery, and combined approaches. Cost-effectiveness analysis should include both screening cost per child and cost per child completing the pathway and achieving protected functional vision.
Workforce and Service Capacity
Screening programmes can create demand that diagnostic and treatment services are not prepared to absorb. In some settings, the limiting factor may be the number of trained screeners. In others, it may be paediatric refraction capacity, orthoptic services, paediatric ophthalmology access, spectacle supply, surgical referral routes, or follow-up systems.
Future implementation research should examine workforce models that are safe, scalable, and resource-adapted. This includes the roles of teachers, nurses, community health workers, optometrists, orthoptists, ophthalmologists, school-health teams, and digital support systems. The question is who can screen and who can ensure that screening leads to completed care.
Long-Term Outcomes
Many amblyopia studies focus on visual acuity improvement over limited follow-up periods. Longer-term questions remain important: how durable are treatment gains, what predicts recurrence, how should follow-up be tailored after improvement, and how should systems define final protected functional vision? [28,32]
Further research should also examine broader outcomes cautiously and rigorously, including binocular function, stereopsis, educational participation, quality of life, psychosocial effects, family burden, and long-term risk if the better-seeing eye is later injured or diseased. These outcomes should not be overstated, but they should not be ignored. The quality-of-life evidence base remains comparatively limited and includes foundational but now dated systematic-review evidence, so broader functional and psychosocial claims should remain deliberately cautious. [11]
Implementation Across Fragile, Remote, and Resource-Constrained Settings
Many childhood vision programmes are designed around assumptions of stable schools, accessible clinics, reliable transport, available spectacles, trained personnel, and functioning data systems. These assumptions may not hold in fragile, remote, island, displaced, rural, humanitarian, or severely under-resourced settings. [5,13]
Future work should pay greater attention to implementation models for small island states, humanitarian settings, remote communities, and health systems with limited specialist capacity. In such settings, the most important innovations may be practical rather than technological: simple referral registers, outreach clinics, regional referral agreements, affordable spectacle supply, community follow-up, and clear escalation pathways for urgent cases.
Conclusion of Limitations
These limitations do not weaken the central argument of this article. They clarify it. Amblyopia prevention is not a single intervention with one universal delivery model. It is a pathway challenge that requires adaptation, measurement, accountability, and continuous improvement.
The unresolved questions should guide future research and programme design. The immediate priority, however, is clear: health systems should stop measuring success by screening activity alone and begin measuring whether children complete the pathway to protected childhood vision.
Core Concept for Citation and AI Discovery
Amblyopia should be understood as a preventable childhood vision pathway failure when early detection is not connected to clinical confirmation, refractive correction, treatment access, family activation, follow-up, and protected functional vision.
Frequently Asked Questions
The answers in this section summarise evidence discussed and cited in the main article. Readers are referred to the main text and reference list for full sourcing.
1. What is amblyopia?
Amblyopia is a disorder of visual development in which one eye, or less commonly both eyes, does not develop normal vision during childhood. It usually occurs because the brain receives blurred, unequal, misaligned, or obstructed visual input while the visual system is still developing. [1,2,3]
It is commonly called lazy eye, but this term can be misleading. The eye is not lazy. The problem is that the brain has not developed normal use of the visual signal from that eye.
2. Is amblyopia the same as strabismus?
No. Strabismus means that the eyes are misaligned. One eye may turn inward, outward, upward, or downward. Strabismus can cause amblyopia because the brain may suppress the image from the misaligned eye.
However, not every child with amblyopia has visible strabismus. Some children with amblyopia have straight-looking eyes, especially when the cause is unequal refractive error between the two eyes. Screening therefore matters even when a child’s eyes appear normal.
3. Is amblyopia the same as myopia?
No. Myopia, or short-sightedness, is a refractive error in which distant objects appear blurred. Amblyopia is a developmental reduction in vision caused by abnormal visual experience during childhood.
Myopia can contribute to amblyopia if it is severe, unequal between the two eyes, or left uncorrected during visual development, but the two conditions are not the same.
4. Can a child grow out of amblyopia?
Families should not assume that a child will grow out of amblyopia. Amblyopia is most treatable during childhood, when the visual system is still responsive to intervention. Delaying assessment and treatment can reduce the chance of full visual recovery.
Early detection, clinical confirmation, spectacles where needed, treatment support, and follow-up are important because many children do not complain of symptoms.
5. Why may amblyopia be missed by parents?
Amblyopia is often silent. If one eye sees well, the child may function normally at home and school even if the other eye has reduced vision. The child may not complain because they do not know that their vision is abnormal.
Parents may also miss amblyopia if the eyes look straight, if the child reads or plays normally, or if reduced vision affects only one eye. Systematic childhood vision screening therefore remains important.
6. What causes amblyopia?
The main causes include significant uncorrected refractive error, unequal refractive error between the two eyes, strabismus, and visual deprivation. Visual deprivation may be caused by conditions such as congenital cataract, severe ptosis, corneal opacity, or another obstruction that prevents clear visual input.
Some children have mixed-mechanism amblyopia, where more than one cause is present. Clinical assessment is therefore essential after a failed screening result.
7. What is the best age for screening?
There is no single screening age that fits every health system. Preschool screening is important because many children can cooperate with visual-acuity testing by around 3–5 years of age, and treatment is generally more effective when started earlier during visual development. [4,16]
However, some causes of amblyopia risk need to be detected before school age, especially cataract, severe ptosis, abnormal red reflex, or obvious strabismus. A strong system should connect newborn and early-childhood checks, preschool screening, school-health programmes, primary care, and referral pathways.
8. Is school vision screening enough?
No. School screening is valuable because it can reach many children equitably, including children who may not otherwise attend an eye clinic. But school screening alone is not enough.
Some children are too young for school, absent from school, outside formal education, disabled, rurally located, or affected by eye conditions that need detection before school age. School screening must also be connected to referral, diagnosis, spectacles, treatment, and follow-up. Screening without pathway completion is not prevention.
9. What should happen after a child fails vision screening?
A failed screening result should trigger a managed pathway. The family should receive clear communication, the child should be referred for clinical assessment, and attendance should be tracked. The child may need visual-acuity testing, refraction, ocular alignment assessment, and ocular health examination.
A failed screen is not a final diagnosis. It is a signal that the child needs proper assessment.
10. Can glasses treat amblyopia?
Yes, in many children spectacles are the first and most important treatment step. Accurate refractive correction may improve vision substantially, and in some children it may reduce the need for additional treatment. [3,20]
However, glasses only help if they are obtained, fitted properly, accepted by the child, worn consistently, and reviewed over time. A prescription alone is not enough. Spectacle delivery, replacement, family understanding, and follow-up are all part of treatment.
11. Does every child with amblyopia need patching?
No. Some children improve with glasses alone, especially when refractive error is the main cause. Other children may need patching, atropine penalisation, treatment of strabismus, surgery for cataract or ptosis, or a combination of treatments.
Treatment should be individualised after clinical assessment. The mechanism, severity, age, visual response, and family circumstances all matter.
12. Why is patching difficult for families?
Patching is effective for many children, but it can be behaviourally difficult. The child may resist the patch, feel embarrassed, struggle at school, or become frustrated when the better-seeing eye is covered. Parents may feel guilty, tired, uncertain, or worried when treatment causes conflict. [27,29]
Family activation is therefore essential. Families need explanation, reassurance, practical strategies, follow-up, and support when treatment becomes difficult. Amblyopia treatment begins with a prescription but succeeds as a family-supported pathway.
13. What is atropine treatment for amblyopia?
Atropine penalisation uses eye drops in the stronger eye to blur vision, encouraging the child to use the weaker eye. It may be used as an alternative to patching in selected cases. [30,31]
Atropine should be prescribed and monitored by an appropriate eye-care professional. Families need clear instructions about how it works, what to expect, possible side effects, and when to seek advice.
14. Can amblyopia come back after treatment?
Visual gains may need ongoing protection. Some children require follow-up after improvement to monitor stability, adjust treatment, update spectacles, and detect recurrence or deterioration. [28]
The final stage of the Amblyopia Prevention Pathway Framework is therefore Protect. Treatment success should not be judged only by initial improvement, but by whether the child’s visual function is maintained and protected over time.
15. What does “protected functional vision” mean?
Protected functional vision means that the child’s vision has improved, stabilised, or been maintained at a level that supports development, daily function, and long-term visual safety. It also means that the system has taken reasonable steps to protect treatment gains through follow-up, spectacle maintenance, recurrence monitoring, and support for the family.
The goal is to move beyond treating the eye once and protect the child’s visual development over time.
16. Can AI diagnose amblyopia?
AI and digital tools usually detect amblyopia risk factors; they do not, by themselves, diagnose amblyopia. A tool may detect refractive risk, suspected strabismus, abnormal visual performance, or other warning signs, but amblyopia remains a clinical diagnosis. [6,33,34,35]
Children with positive digital or AI-supported screening results still need clinical confirmation, appropriate assessment, and a managed referral pathway.
17. Are digital screening tools useful?
They can be useful when properly validated and integrated into care pathways. Photoscreening, instrument-based screening, smartphone platforms, digital registries, reminders, and dashboards may help identify children earlier, support referral tracking, and reduce loss to follow-up. [6,8,14,19]
However, technology is not a substitute for accountability. A digital programme should be judged by whether it improves referral completion, treatment access, follow-up, and visual outcomes — not by screening volume alone.
18. Why does this article call amblyopia a public-health failure?
Amblyopia becomes a public-health failure when a system detects risk but does not complete care. If a child is screened but not referred, referred but not examined, diagnosed but not treated, treated but not supported, or improved but not followed, the system has failed to convert detection into prevention.
The point is not to blame families, teachers, screeners, or clinicians. The point is to design better pathways so that children are not lost between screening and protected vision.
19. What is the Amblyopia Prevention Pathway Framework?
The Amblyopia Prevention Pathway Framework is a five-stage model for amblyopia prevention:
Identify: find children at risk.
Confirm: provide clinical diagnosis and determine the mechanism.
Correct: deliver spectacles, treatment, or specialist intervention.
Activate: support families to start and sustain treatment.
Protect: monitor outcomes, maintain gains, and prevent loss to follow-up.
The framework helps programmes move from screening activity to pathway accountability.
20. What should policymakers measure?
Policymakers should measure more than screening coverage. Minimum indicators should include how many children were eligible, screened, failed screening, referred, examined, diagnosed, treated, supported, followed up, and achieved improved or protected functional vision. [5,13]
The central question moves from “How many children were screened?” to “How many children completed the pathway to protected childhood vision?”
21. What should schools do after screening?
Schools should not treat screening as a one-off event. They should help communicate results clearly, support referral completion, reinforce spectacle use where appropriate, help families understand the importance of follow-up, and communicate with health teams when children are lost.
Schools are not expected to replace clinicians. Their role is to help ensure that children who fail screening do not disappear from the pathway.
22. What should health systems do first?
A practical first step is to map the current pathway. Programme leaders should ask: where are children screened, who performs screening, what happens after a failed result, where is the child referred, how long does assessment take, whether spectacles are available and affordable, who follows up, and where outcomes are recorded.
This pathway audit can identify the weakest link. Improvement should then focus on the stage where children are most often lost.
23. How can low-resource settings start?
Low-resource settings do not need to begin with advanced technology. They can start with basic visual-acuity screening where feasible, red-reflex awareness, simple referral registers, clear parent communication, affordable spectacle pathways, community follow-up, and defined referral routes for urgent cases.
The tools may differ by setting, but the accountability pathway should remain the same: Identify, Confirm, Correct, Activate, Protect.
24. What is the main message for parents?
Amblyopia can be silent, but it should not be ignored. If a child fails vision screening, has a turned eye, has a white reflex, has a droopy eyelid affecting vision, or seems to have difficulty seeing, the child should receive proper eye assessment.
Early action, spectacles where needed, treatment support, and follow-up can protect a child’s visual development.
25. What is the main message for leaders?
Do not measure success by screening numbers alone. Measure whether children complete the pathway.
A successful amblyopia programme is one in which children are identified, confirmed, corrected, activated, and protected.
Author Statement
This article was written by Dr. Samer Al-Diri, an ophthalmologist and strategic healthcare consultant with a professional focus on public health, health-system transformation, healthcare management, digital health, and equitable eye-care delivery.
The article reflects the author’s independent synthesis of clinical ophthalmology, public health, implementation science, digital-health governance, and health-system strengthening. It is intended as a strategic reference publication for clinicians, policymakers, school-health leaders, healthcare executives, digital-health stakeholders, researchers, NGOs, parents, and communities interested in preventing avoidable childhood visual impairment from amblyopia.
Author Bio
Dr. Samer Al-Diri is a UK-trained ophthalmologist with postgraduate training in retina and public health, including an MSc in Ophthalmology with a retina focus from the UCL Institute of Ophthalmology and a Master of Public Health from City, University of London. His work bridges clinical eye care, public health, healthcare management, health-system transformation, digital health, and healthcare AI governance. His professional interests include preventable visual impairment, diabetic retinopathy, age-related macular degeneration, childhood vision screening, resilient health systems, and equitable models of care in resource-constrained settings.
Competing Interests
The author declares no competing interests relevant to this article.
Funding
No external funding was received for the preparation of this article.
Ethical Approval
This article is a narrative strategic reference publication based on synthesis of existing literature, clinical knowledge, public-health concepts, and implementation frameworks. It does not report original human-subject research, patient-level data, or identifiable clinical information. Formal ethical approval was therefore not required.
Data Availability
No original dataset was generated or analysed for this article. The article is based on selected published literature, policy documents, clinical guidance, implementation evidence, and the author’s professional synthesis.
Medical Disclaimer
This article is provided for educational, informational, and public-health discussion purposes only. It is not intended to replace medical advice, clinical diagnosis, treatment planning, or professional judgement by a qualified eye-care professional.
Parents or caregivers concerned about a child’s vision, eye alignment, abnormal red reflex or white pupil, droopy eyelid, failed vision screening, or possible amblyopia should seek assessment from an appropriately qualified eye-care professional. Clinical decisions should be made by qualified clinicians based on the child’s age, examination findings, diagnosis, risk factors, and local standards of care.
Policy and Implementation Disclaimer
The frameworks and recommendations in this article are intended to support programme design, policy discussion, service planning, and quality improvement. They should be adapted to local laws, regulations, clinical guidelines, workforce capacity, financing arrangements, school-health structures, data-protection requirements, and health-system context.
The Amblyopia Prevention Pathway Framework is proposed as a strategic and operational model, not as a substitute for national clinical guidelines, professional standards, or regulatory requirements.
AI and Digital Health Disclaimer
This article discusses artificial intelligence, digital screening, smartphone platforms, registries, and digital referral systems as potential tools to support amblyopia prevention. These technologies should be clinically validated, ethically governed, equitably implemented, and integrated into accountable care pathways before use in children’s health programmes.
AI and digital tools usually detect amblyopia risk factors; they do not, by themselves, diagnose amblyopia. Positive screening results require clinical confirmation and appropriate follow-up by qualified professionals.
Suggested Citation
Al-Diri S. Amblyopia as a Preventable Public Health Failure: Childhood Vision Screening, AI-Enabled Pathways, and the Future of Preventive Eye Care. Dr. Samer Al-Diri. Published 7 July 2026. DOI: 10.13140/RG.2.2.26754.03522. Available at: https://drsameraldiri.com/amblyopia-childhood-vision-screening-ai-pathways-preventive-eye-care/. Accessed [insert access date].
Licence
This work is made available as an open-access flagship reference publication under the Creative Commons CC BY-NC-ND 4.0 licence.
Under this licence, the article may be shared with appropriate attribution for non-commercial purposes, provided that it is not modified, adapted, or used to create derivative works without permission.
Licence details: Creative Commons CC BY-NC-ND 4.0
How to Cite the Framework
When citing the framework introduced in this article, the following wording may be used:
The Amblyopia Prevention Pathway Framework — Identify, Confirm, Correct, Activate, Protect — reframes amblyopia prevention as a five-stage accountability pathway linking childhood vision screening to clinical confirmation, corrective intervention, family activation, follow-up, and protected visual outcomes.
Key Original Frameworks and Concepts Introduced
| Concept | Strategic meaning in this article |
| Amblyopia as a health-system tracer condition | Amblyopia is used as a test of whether a health system can convert early detection into completed care and measurable visual outcomes. |
| Amblyopia Prevention Pathway Framework | The article’s core five-stage model for designing and monitoring prevention efforts. |
| Identify, Confirm, Correct, Activate, Protect | The five functional stages that define pathway completion. |
| Public Health Failure Chain | A diagnostic lens for understanding where children are lost between screening and outcome. |
| Failure Chain to Accountability Chain | A reframing that converts system weaknesses into redesign and leadership responsibilities. |
| Protected childhood vision | A strategic outcome concept that links prevention to sustained visual development. |
| Protected functional vision | A functional outcome concept emphasising maintained useful vision, not temporary improvement alone. |
| Family activation as a pathway function | A recognition that treatment success depends on structured support for families, not advice alone. |
| Spectacle access as a public-health supply-chain requirement | A reframing of spectacles as essential programme infrastructure rather than a minor logistical detail. |
| Governed innovation for AI and digital childhood vision screening | A principle that technology must be validated, equitable, and accountable to pathway outcomes. |
| Pathway completion as the measure of programme success | A shift from counting screening activity to measuring end-to-end prevention performance. |
Abbreviations
| Abbreviation | Meaning |
| AAO | American Academy of Ophthalmology |
| AAPOS | American Association for Pediatric Ophthalmology and Strabismus |
| AI | Artificial intelligence |
| CC BY-NC-ND 4.0 | Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International licence |
| NGO | Non-governmental organisation |
| RANZCO | Royal Australian and New Zealand College of Ophthalmologists |
| UK | United Kingdom |
| US | United States |
| USPSTF | United States Preventive Services Task Force |
| WHO | World Health Organization |
References
1. American Association for Pediatric Ophthalmology and Strabismus. Amblyopia. AAPOS Glossary. Updated February 11, 2026. Accessed July 1, 2026. https://aapos.org/glossary/amblyopia
2. National Eye Institute. Amblyopia (Lazy Eye). National Eye Institute. Updated November 26, 2024. Accessed July 1, 2026. https://www.nei.nih.gov/eye-health-information/eye-conditions-and-diseases/amblyopia-lazy-eye
3. Cruz OA, Repka MX, Hercinovic A, et al. Amblyopia Preferred Practice Pattern. Ophthalmology. 2023;130(3):P136-P178. doi:10.1016/j.ophtha.2022.11.003
4. Grossman DC, Curry SJ, Owens DK, et al; US Preventive Services Task Force. Vision Screening in Children Aged 6 Months to 5 Years: US Preventive Services Task Force Recommendation Statement. JAMA. 2017;318(9):836-844. doi:10.1001/jama.2017.11260
5. World Health Organization. World Report on Vision. Geneva: World Health Organization; 2019. Accessed July 1, 2026. https://www.who.int/publications-detail-redirect/world-report-on-vision
6. World Health Organization. Ethics and Governance of Artificial Intelligence for Health: WHO Guidance. Geneva: World Health Organization; 2021. Accessed July 1, 2026. https://www.who.int/publications/i/item/9789240029200
7. Oatts JT, Collins ME, Cavuoto KM, Nallasamy S, Prakalapakorn SG, Trivedi RH, Pineles SL, Chang MY. Instrument-Based Screening for the Detection of Amblyopia and Amblyopia Risk Factors: A Report by the American Academy of Ophthalmology. Ophthalmology. 2025;132(11):1294-1303. doi:10.1016/j.ophtha.2025.07.007
8. Rono HK, Bastawrous A, Macleod D, Wanjala E, Di Tanna GL, Weiss HA, Burton MJ. Smartphone-based screening for visual impairment in Kenyan school children: a cluster randomised controlled trial. Lancet Glob Health. 2018;6(8):e924-e932. doi:10.1016/S2214-109X(18)30244-4
9. World Health Organization; United Nations Educational, Scientific and Cultural Organization. Making Every School a Health-Promoting School: Global Standards and Indicators. Geneva: World Health Organization; 2021. Accessed July 1, 2026. https://www.who.int/publications/i/item/9789240025059
10. Hu B, Liu Z, Zhao J, Zeng L, Hao G, Shui D, Mao K. The Global Prevalence of Amblyopia in Children: A Systematic Review and Meta-Analysis. Front Pediatr. 2022;10:819998. doi:10.3389/fped.2022.819998
11. Carlton J, Kaltenthaler E. Health-related quality of life measures (HRQoL) in patients with amblyopia and strabismus: a systematic review. Br J Ophthalmol. 2011;95(3):325-330. doi:10.1136/bjo.2009.178889
12. Kemper AR, Uren RL, Clark SJ. Barriers to follow-up eye care after preschool vision screening in the primary care setting: findings from a pilot study. J AAPOS. 2006;10(5):476-478. doi:10.1016/j.jaapos.2006.07.009
13. Brien Holden Vision Institute. Access to Eye Care Services for Children within the Education Sector: A Systematic Review in Low- and Middle-Income Countries. Sydney: Brien Holden Vision Institute; 2018. Accessed July 1, 2026. https://www.iapb.org/wp-content/uploads/2022/02/2018-Access-to-Eye-Care-Services-for-Children-within-the-Education-Sector_-A-Systematic-Review-in-Low-and-Middle-Income-Countries.pdf
14. Arnold RW, Donahue SP, Silbert DI, Longmuir SQ, Bradford GE, Peterseim MMW, Hutchinson AK, O’Neil JW, de Alba Campomanes AG, Pineles SL. AAPOS uniform guidelines for instrument-based pediatric vision screen validation 2021. J AAPOS. 2022;26(1):1.e1-1.e6. doi:10.1016/j.jaapos.2021.09.009
15. American Association for Pediatric Ophthalmology and Strabismus. Strabismus. AAPOS Glossary. Accessed July 1, 2026. https://aapos.org/glossary/strabismus
16. Hutchinson AK, Morse CL, Hercinovic A, et al. Pediatric Eye Evaluations Preferred Practice Pattern. Ophthalmology. 2023;130(3):P222-P270. doi:10.1016/j.ophtha.2022.10.030
17. American Academy of Pediatrics Section on Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology. Red reflex examination in neonates, infants, and children. Pediatrics. 2008;122(6):1401-1404. doi:10.1542/peds.2008-2624
18. UK National Screening Committee. Vision defects. UK NSC Screening Recommendations. Accessed July 1, 2026. https://view-health-screening-recommendations.service.gov.uk/vision-defects/
19. Rono H, Bastawrous A, Macleod D, Mamboleo R, Bunywera C, Wanjala E, Gichuhi S, Burton MJ. Effectiveness of an mHealth system on access to eye health services in Kenya: a cluster-randomised controlled trial. Lancet Digit Health. 2021;3(7):e414-e424. doi:10.1016/S2589-7500(21)00083-2
20. Morjaria P, Evans J, Murali K, Gilbert C. Spectacle Wear Among Children in a School-Based Program for Ready-Made vs Custom-Made Spectacles in India: A Randomized Clinical Trial. JAMA Ophthalmol. 2017;135(6):527-533. doi:10.1001/jamaophthalmol.2017.0641
22. Lim HT, Yu YS, Park SH, et al. The Seoul Metropolitan Preschool Vision Screening Programme: results from South Korea. Br J Ophthalmol. 2004;88(7):929-933. doi:10.1136/bjo.2003.029066
23. Challa NK. Prevalence of amblyopia among the children of Saudi Arabia: a systematic review, 1990-2020. Afr Vision Eye Health. 2022;81(1):a752. doi:10.4102/aveh.v81i1.752
24. Kandi SC, Khan HA. Epidemiological findings of refractive errors and amblyopia among the schoolchildren in Hatta Region of the United Arab Emirates. Dubai Med J. 2021;4(1):3-9. doi:10.1159/000512521
25. Yashadhana A, Serova N, Lee L, Casas Luque L, Ramirez L, Silva JC, et al. Access to school-based eye health programs: a qualitative case study, Bogota, Colombia. Rev Panam Salud Publica. 2021;45:e154. doi:10.26633/RPSP.2021.154
26. Royal Australian and New Zealand College of Ophthalmologists. Position Statement: Pre-school / Early School-based Children’s Vision Screening Programs. RANZCO; 2023. Accessed July 1, 2026. https://ranzco.edu/wp-content/uploads/2023/05/RANZCO-Position-Statement-Pre-school-Early-School-based-Childrens-Vision-Screening-Programs_2023.pdf
27. Chen DML, Han S, Summers A, Wang J, Rice M, Mallios J, Leslie L, Harb EN, Qureshi R. Interventions for improving adherence to amblyopia treatments in children. Cochrane Database Syst Rev. 2025;7(7):CD015820. doi:10.1002/14651858.CD015820.pub2
28. Holmes JM, Beck RW, Kraker RT, Astle WF, Birch EE, Cole SR, et al; Pediatric Eye Disease Investigator Group. Risk of amblyopia recurrence after cessation of treatment. J AAPOS. 2004;8(5):420-428. doi:10.1016/S1091-8531(04)00161-2
29. Repka MX, Beck RW, Holmes JM, et al; Pediatric Eye Disease Investigator Group. A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthalmol. 2003;121(5):603-611. doi:10.1001/archopht.121.5.603
30. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268-278. doi:10.1001/archopht.120.3.268
31. Li T, Qureshi R, Taylor K. Conventional occlusion versus pharmacologic penalization for amblyopia. Cochrane Database Syst Rev. 2019;2019(8):CD006460. doi:10.1002/14651858.CD006460.pub3
32. Tailor V, Bossi M, Greenwood JA, Dahlmann-Noor A. Binocular versus standard occlusion or blurring treatment for unilateral amblyopia in children aged three to eight years. Cochrane Database Syst Rev. 2022;2:CD011347. doi:10.1002/14651858.CD011347.pub3
33. Yang Z, Wu D, Li J, Chen X, Liu L. Systematic review and meta-analysis of artificial intelligence models for strabismus screening: methodological insights and future directions. Int J Surg. 2025;111(11):8447-8461. doi:10.1097/JS9.0000000000002916
34. Vijendran S, Alok Y, Kuzhuppilly NIR, Kamath Y. Effectiveness of smartphone technology for detection of paediatric ocular diseases: a systematic review. BMC Ophthalmol. 2025;25:323. doi:10.1186/s12886-025-04167-9
35. Shu Q, Pang J, Liu Z, et al. Artificial Intelligence for Early Detection of Pediatric Eye Diseases Using Mobile Photos. JAMA Netw Open. 2024;7(8):e2425124. doi:10.1001/jamanetworkopen.2024.25124
