Preserving Sight in an Ageing World
Production Edition V11.0
TABLE OF CONTENTS
Open Access Reference Publication
Author: Dr. Samer Al-Diri
Author ORCID iD: 0009-0004-1908-0714 | https://orcid.org/0009-0004-1908-0714
Licence: Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Al-Diri S. Age-Related Macular Degeneration: Population Ageing, Health-System Impact, Artificial Intelligence, and the Future of Sustainable Vision Care — Preserving Sight in an Ageing World. DrSamerAlDiri.com. Published 23 June 2026. Available at: https://drsameraldiri.com/age-related-macular-degeneration-population-ageing-health-system-impact-artificial-intelligence-and-the-future-of-sustainable-vision-care/. Accessed 23 June 2026.
Related flagship publications: This article should be read alongside my flagship publication on diabetic retinopathy, artificial intelligence, and preventable blindness, and my executive reference publication on healthcare AI governance and patient-centred accountability.
Front Matter
2. Methods Statement – Evidence Synthesis
3. Author’s Note – Why I Wrote This
4. Executive Summary for Policymakers
5. Key Messages
Part I – Frameworks
7. Introduction
9. The Sustainable Vision Care Framework (including The Vision Dividend)
Part II – Epidemiology and Human Impact
10. AMD and the Global Burden of Population Ageing
11. The Human Impact of Age-Related Macular Degeneration
Part III – Health Systems and Workforce
12. Health-System Impact of Age-Related Macular Degeneration
13. Geographic Atrophy: The New Therapeutic Era and the Challenge of Meaningful Benefit (including Structure–Function Challenge and safety discussion)
14. Evidence-Based Hope in AMD
15. Workforce Pressures, Capacity Constraints, and the Vision-Care Capacity Gap
Part IV – Technology and Future Models
17. Artificial Intelligence and the Future of AMD Care
18. From Reactive Care to Future-Ready Vision Systems
Part V – Looking Ahead
19. The Future of AMD Care (Seven Forecasts)
20. Executive Recommendations for Health-System Leaders and Policymakers
21. Adapting Sustainable Vision Care Across Diverse Health‑System Contexts
22. Call to Action
23. Final Reflection: The Future of Vision in an Ageing World
Back Matter
– Open Access Licensing Statement
– References (75 entries)
– List of Figures
Executive visual abstract. Age-related macular degeneration in an ageing world: a global health-system imperative linking individual dignity, clinic care, health-system capacity, ageing society, and global policy.
Executive Abstract
By 2040, nearly 300 million people may be living with age-related macular degeneration (AMD). That number should make every health system pause. AMD is still a retinal disease, but it is also becoming a test of how ageing societies preserve reading, face recognition, mobility, confidence, and independence across longer lives. Globally, AMD already affects more than 200 million people, and demographic ageing is expected to increase this burden over coming decades [2].
Demographic change is fundamentally altering the future burden of AMD. As populations live longer, the number of individuals at risk of developing AMD continues to increase. That tension is what I describe as the Longevity–Vision Paradox: the same advances in healthcare and public health that extend lifespan also increase the number of years during which people may live with age-related visual impairment. AMD therefore belongs not only in ophthalmology clinics, but also in healthy-ageing policy and health-system strategy.
Framing vision as a core component of healthy ageing — alongside mobility, cognition, cardiovascular health, and social participation — helps explain why preserving sight matters far beyond ophthalmology. Vision loss changes how people read, move, recognise faces, manage daily tasks, and stay connected. For patients, preserving vision is often about preserving a life that still feels familiar: the newspaper, the medicine label, the face across the table, the confidence to leave home alone.
Geographic Atrophy (GA), the advanced atrophic form of AMD, deserves particular attention. For years it represented one of retinal medicine’s most difficult conversations: a clear diagnosis, progressive tissue loss, and little to offer beyond monitoring and support. Disease-modifying therapies have changed that conversation. They have also brought harder questions about meaningful benefit, safety, regulatory divergence, workforce capacity, equity, and affordability.
Workforce Mathematics, the Implementation Chasm, Vision-System Resilience, and the Vision-Care Capacity Gap frame a practical reality: scientific progress alone does not guarantee patient benefit. A therapy can be effective, approved, and funded — and still fail patients if clinics lack the people, imaging capacity, governance, financing, and delivery pathways to provide it.
Artificial intelligence now sits across the AMD pathway: image analysis, progression prediction, personalised monitoring, treatment prioritisation, and future virtual retina-care models. Its promise is real. So are its limits. In AMD, AI should augment clinicians and health systems, not replace them.
A sustainable vision-care lens brings these issues together: prevention, early detection, treatment, rehabilitation, workforce development, technology, and health-system preparedness. The future challenge is not simply developing better treatments. It is making sure that scientific advances reach people in ways that are meaningful, equitable, and sustainable.
The central argument is that AMD has become a global test case for ageing societies. How well health systems preserve vision will influence independence, participation, quality of life, and the credibility of healthy-ageing strategies. The lessons extend beyond ophthalmology into healthcare transformation, health-system strengthening, and sustainable care delivery.
The aim is practical: to help clinicians, policymakers, healthcare leaders, and public-health professionals prepare for the next phase of AMD care in ageing societies.
Methods Statement – Evidence Synthesis
I approached this as a narrative evidence synthesis, not a formal systematic review. The evidence base included peer-reviewed literature, global health reports, regulatory documents, clinical trial registries, and health-system policy sources. In March–May 2026, I searched PubMed, the Cochrane Library, and Google Scholar using terms related to age-related macular degeneration, geographic atrophy, epidemiology, workforce capacity, artificial intelligence, health systems, implementation, and healthy ageing. I prioritised systematic reviews, randomised trials, large observational studies, WHO and Lancet Global Health reports, and regulatory assessments from agencies such as the FDA, EMA, NICE, and other public authorities. Where the evidence is uncertain, I have tried to say so plainly. Strategic targets in this article should be read as illustrative planning goals unless a specific citation supports them. I drafted the substantive conclusions myself; artificial intelligence tools assisted with language refinement, formatting, and editorial organisation only.
The conceptual language used here is intended to clarify, not to overclaim. Two terms are presented as original contributions: the Longevity–Vision Paradox and the Geographic Atrophy Transition Era. Other terms — the Vision Dividend, Implementation Chasm, Workforce Mathematics, Structure–Function Challenge, Vision-Care Capacity Gap, Ageing Vision System, Sustainable Vision Care Framework, and Vision-System Resilience — are used as descriptive or integrative lenses. They help organise the argument, but they should not be mistaken for rigid models or proprietary claims.
Author’s Note – Why I Wrote This
I wrote this work because I kept seeing the same pattern repeat: science moving forward while systems struggled to keep pace. Patients waited. Clinicians absorbed the pressure. Administrators were sometimes surprised by demand that was, in truth, predictable.
My perspective is shaped by working across different health-system environments. In the United Kingdom, I saw how sophisticated retinal services can still be stretched by volume and workforce pressure. In the United Arab Emirates, rapid health-system development shows how quickly infrastructure and ambition can evolve. In humanitarian and South Pacific settings, the problem may begin much earlier: the absence of a scan, a delayed referral, or the long journey to a specialist clinic.
The AMD challenge looks different in each setting, but the patient’s fear is remarkably similar. Losing sight means losing confidence, independence, and sometimes identity. That is why the central question is not only what retina science can achieve. It is what health systems are prepared to deliver.
A Note on Scope and Humility
The frameworks in this work are deliberately descriptive. They are not clinical guidelines, and they should not be read as universal prescriptions. The Longevity–Vision Paradox, for example, simplifies a complex interaction between ageing, multimorbidity, health financing, culture, geography, and patient preference. It is useful because it makes the tension visible, not because it explains every setting equally well.
I am also conscious that my own experience, while international, cannot fully represent the realities of every low- and middle-income country or every local health system. Readers should adapt the ideas to their own context. The goal is to provoke better planning, more honest debate, and more patient-centred implementation.
Executive Summary for Policymakers
Why This Matters Now
Age-related macular degeneration (AMD) and its advanced form, Geographic Atrophy (GA), are not merely retinal diseases. They are defining challenges of ageing societies. As populations live longer, preserving vision becomes increasingly central for maintaining independence, participation, wellbeing, and healthy ageing. Without proactive action, the growing burden of AMD will place increasing pressure on healthcare systems, workforces, and public finances.
The evidence presented in this work suggests that AMD increasingly serves as a global test case for how ageing societies preserve vision, independence, and quality of life across longer lifespans. Scientific innovation is advancing rapidly, but innovation alone will not guarantee patient benefit. Sustainable success will depend on whether healthcare systems can translate innovation into equitable access, workforce readiness, and meaningful outcomes.
Five Strategic Priorities for Policymakers and Health-System Leaders
1. Integrate Vision into Healthy-Ageing Strategies – Recognise vision preservation as a core pillar of healthy ageing alongside mobility, cognition, cardiovascular health, and social participation. National healthy-ageing frameworks should incorporate vision-related indicators and eye-health objectives.
2. Strengthen Workforce Capacity and Service Resilience – Expand ophthalmology workforce capacity, support multidisciplinary models of care, and align workforce planning with projected demographic demand and future treatment requirements.
3. Prioritise Early Detection, Risk Stratification, and Prevention – Strengthen AMD awareness, promote risk-factor modification, and develop targeted surveillance pathways for high-risk populations to support earlier intervention and improved outcomes.
4. Develop Equitable and Sustainable Access to Emerging Therapies – Establish evidence-based access pathways for Geographic Atrophy therapies supported by transparent health-technology assessment, real-world outcome monitoring, and ongoing evaluation of patient benefit and value.
5. Deploy Artificial Intelligence Responsibly – Implement AI-enabled retinal care within well-designed governance frameworks that prioritise validation, transparency, equity, privacy protection, and continuous performance monitoring.
GUIDING PRINCIPLE
Scientific innovation alone will not determine the future of AMD care. The future will be shaped by whether healthcare systems can convert innovation into sustainable, equitable, and meaningful patient benefit.
Potential Benefits
Implementation of these priorities could help preserve independence, mobility, reading ability, and quality of life for millions of older adults while reducing avoidable vision loss and strengthening health-system resilience.
The resulting Vision Dividend would extend beyond ophthalmology, contributing to healthier ageing, reduced care dependency, improved population wellbeing, and broader societal and economic benefits.
The cost of inaction is progressive vision loss, widening inequalities, increasing workforce pressures, and avoidable loss of independence among ageing populations. The opportunity to act is now.
Key Messages
The core message is simple, but uncomfortable: AMD is no longer only a specialist retinal condition. It is becoming one of the defining tests of ageing societies. Longer lives will bring more AMD, more Geographic Atrophy, more imaging, more monitoring, more treatment decisions, and more pressure on already stretched eye-care services.
Preserving vision should therefore sit alongside mobility, cognition, cardiovascular health, and social participation as part of healthy ageing policy. Patients do not experience AMD as a lesion on a scan. They experience it as lost reading, missed faces, reduced confidence, anxiety about the future, and a gradual narrowing of ordinary life. That is why functional outcomes, rehabilitation, independence, and quality of life must remain central.
GA therapies, AI-enabled retinal care, home monitoring, and regenerative approaches all create genuine hope. Yet hope is not implementation. Scientific progress must pass through workforce capacity, reimbursement, governance, infrastructure, safety monitoring, and equity before it becomes real benefit for patients. This is where the gap between discovery and delivery becomes visible.
For policymakers and health-system leaders, AMD offers a wider lesson. The future of care will depend not only on better molecules or smarter algorithms, but on whether systems can deliver sight-preserving services fairly, safely, and sustainably at population scale.
Reader’s Guide
The intended audience includes clinicians (retina specialists and ophthalmologists), healthcare leaders and policymakers, public-health and digital-health professionals, researchers, and readers interested in healthy ageing and sustainable vision care.
AMD is often viewed primarily as a retinal disease. That remains true — but incomplete. The pages that follow treat AMD as a clinical challenge, a public-health priority, a healthy-ageing issue, a healthcare-management problem, and a test case for how health systems adapt to chronic disease in older populations.
For Clinicians and Retina Specialists – The sections on AMD pathophysiology, Geographic Atrophy, emerging therapies, regulatory developments, artificial intelligence, and future treatment pathways may be of particular relevance.
For Policymakers and Public-Health Leaders – The sections addressing population ageing, health-system impact, workforce capacity, health equity, healthy ageing, and sustainable vision care may be especially useful.
For Healthcare Executives and Managers – The Workforce Mathematics Model, Implementation Chasm, Vision-System Resilience, and Sustainable Vision Care Framework sections focus on operational, strategic, and organisational implications for future vision-care services.
For Digital Health and Artificial Intelligence Leaders – The sections exploring artificial intelligence, predictive analytics, personalised monitoring, and future models of retina care examine how emerging technologies may influence AMD management and healthcare delivery.
For Patients, Families, and Caregivers – The sections discussing disease impact, treatment developments, quality of life, and Evidence-Based Hope may be particularly valuable for understanding current challenges and future opportunities in AMD care.
Structure of the Article – Five interconnected themes guide the discussion:
1. AMD and the Challenge of Ageing Societies – outlines the growing burden of AMD and presents The Ageing Vision System and the Longevity–Vision Paradox.
2. The Human and Health-System Impact of AMD – examines consequences for patients, caregivers, healthcare services, and workforce planning.
3. Geographic Atrophy and the Future of Vision Care – provides in-depth exploration of GA, emerging therapies, regulatory developments, AI, and workforce implications.
4. Sustainable Vision Care in the Twenty-First Century – presents The Sustainable Vision Care Framework and explores prevention, early detection, treatment, rehabilitation, workforce, technology, and resilience.
5. Future Directions – explores forecasts, healthcare adaptation, emerging technologies, implementation challenges, and the future of sustainable vision care.
A Note on Terminology
Several conceptual frameworks and analytical lenses appear throughout the discussion. Two concepts are identified as original contributions by the author: the Longevity–Vision Paradox and the Geographic Atrophy Transition Era. They are offered as ways of thinking about population ageing, vision loss, and health-system preparedness. Other terms — Vision Dividend, Implementation Chasm, Workforce Mathematics, the Structure–Function Challenge, Vision-Care Capacity Gap, Ageing Vision System, Sustainable Vision Care Framework, and Vision-System Resilience — are used descriptively or integratively. They are not presented as proprietary labels.
A Note on Limits and Interpretation
These frameworks are descriptive, not prescriptive. They simplify complicated realities in order to make them easier to discuss, and that simplification has limits. The Longevity–Vision Paradox may not capture every demographic pathway. The Implementation Chasm may look too linear in systems where politics, financing, professional culture, and patient behaviour interact unpredictably. I am also conscious that my experience across the UK, UAE, humanitarian settings, and the South Pacific cannot fully represent every LMIC or regional reality. The frameworks should therefore be read as tools for discussion, not as final answers.
Patient vignettes used here are anonymised and composite. They are included to make clinical and health-system issues more tangible, not to identify any individual patient.
The central message is simple: the future challenge of AMD is not only to develop better treatments. It is to ensure that ageing societies can deliver effective, equitable, and sustainable vision care to those who need it most.
Introduction
Why Age-Related Macular Degeneration Matters in the Twenty-First Century
Age-related macular degeneration (AMD) is one of the leading causes of irreversible visual impairment worldwide [1] and represents a defining challenge for healthcare systems, policymakers, clinicians, and ageing societies. Historically, AMD has often been viewed primarily as a retinal disease managed within specialist ophthalmic services. While this clinical perspective remains essential, it is no longer sufficient.
The twenty-first century is witnessing an unprecedented demographic transformation. Advances in healthcare, public health, and socioeconomic development have extended life expectancy globally – one of humanity’s greatest achievements. However, as populations live longer, the number of individuals vulnerable to age-related diseases, including AMD, continues to rise.
AMD is not merely becoming more common because populations are growing. It matters more because societies are ageing. The disease now sits at the intersection of ophthalmology, healthy ageing, public health, healthcare management, and health-system sustainability.
Visual function plays a central role in maintaining independence throughout later life. Reading, face recognition, mobility, driving, medication management, financial administration, social participation, and many activities of daily living depend upon the preservation of vision. Vision loss therefore affects far more than the eye alone. It influences quality of life, mental wellbeing, social engagement, physical function, and an individual’s ability to live independently.
For many patients, the consequences of AMD extend beyond visual impairment. The disease may reduce independence, alter relationships, contribute to social isolation, and create substantial emotional and practical burdens for both patients and caregivers. These effects are often difficult to capture through traditional clinical metrics yet represent some of the outcomes that matter most to patients.
At the population level, the implications are equally significant. AMD contributes to increasing demand for ophthalmic services, retinal imaging, specialist workforce capacity, rehabilitation services, and long-term support systems. As therapeutic innovation accelerates, healthcare systems must also prepare for new demands associated with treatment delivery, monitoring, implementation, and equitable access. Scientific progress therefore creates not only opportunities but also new organisational and operational challenges.
The emergence of disease-modifying therapies for Geographic Atrophy, advances in retinal imaging, developments in artificial intelligence, and progress in regenerative medicine have further transformed the AMD landscape. These developments suggest that AMD serves as a model for understanding how health systems respond to innovation within the context of ageing populations. The challenge is no longer simply to diagnose disease or preserve vision. The challenge is to ensure that scientific advances can be translated into meaningful, equitable, and sustainable patient benefit.
Unlike traditional disease-focused reviews, this work places AMD within the broader context of healthy ageing, health-system capacity, workforce mathematics, healthcare transformation, and the implementation challenges that determine whether innovation reaches patients in real-world settings.
AMD is examined here through a broader lens than has traditionally been applied. Rather than viewing it solely as a retinal disorder, the discussion considers AMD as:
– A challenge of population ageing.
– A determinant of healthy ageing and independence.
– A public-health priority.
– A healthcare-management and workforce challenge.
– A test case for healthcare transformation.
– An emerging field for artificial intelligence and digital innovation.
– A strategic opportunity to develop more sustainable models of vision care.
Several concepts help organise the argument, including the Ageing Vision System, the Geographic Atrophy Transition Era, the Structure–Function Challenge, Workforce Mathematics, the Implementation Chasm, Vision-System Resilience, the Vision Dividend, and the Sustainable Vision Care Framework. They are used as practical lenses rather than as rigid models: ways of connecting demographic change, clinical innovation, healthcare delivery, workforce capacity, and health-system preparedness.
The central perspective of this work is straightforward but increasingly central: the future challenge of AMD is not simply to develop better treatments. It is to ensure that ageing societies possess the capacity, workforce, infrastructure, governance, and strategic vision required to deliver effective, equitable, and sustainable care to growing populations at risk of vision loss.
In this sense, AMD represents more than a retinal disease. It offers a lens through which to examine the broader challenges of healthy ageing, healthcare transformation, and sustainable care delivery in the twenty-first century.
The Ageing Vision System
Reframing Vision as a Core Pillar of Healthy Ageing
Introduction
The twenty-first century is defined by population ageing. Advances in healthcare, public health, education, nutrition, sanitation, and socioeconomic development have contributed to substantial gains in life expectancy across much of the world. These achievements represent one of humanity’s greatest successes. Yet they also create new challenges for individuals, healthcare systems, and societies.
Among these challenges is the growing burden of age-related visual impairment.
According to the World Health Organization, at least 2.2 billion people worldwide live with a near or distance vision impairment, of whom at least one billion have a condition that could have been prevented or has yet to be addressed [1]. As populations continue to age, the burden of visual impairment is expected to increase further.
Age-related macular degeneration (AMD), one of the leading causes of irreversible visual impairment worldwide, exemplifies why this challenge is becoming increasingly central [3,4].
Historically, healthy-ageing discussions have focused primarily on mobility, cognition, cardiovascular health, frailty, and social participation. These domains are rightly recognised as major determinants of wellbeing in later life. However, vision has often received comparatively less attention despite its fundamental contribution to nearly every aspect of daily functioning [1].
This relative under-recognition of vision within healthy-ageing policy has attracted increasing attention. The Lancet Global Health Commission on Global Eye Health argued that eye health should be recognised as a central component of healthy ageing, wellbeing, education, productivity, and social participation. These observations support the proposition that preserving vision should be considered a strategic healthy-ageing objective rather than solely a specialist ophthalmic concern [59].
Framing vision as a central component of healthy ageing — what I describe as an ageing vision system — helps clarify why preserving sight should sit alongside mobility and cognition as a strategic objective for ageing societies.
Vision is not merely a sensory function. It is an enabling function. Through vision, individuals navigate their environments, recognise faces, read information, manage medications, maintain social relationships, participate in communities, and preserve independence. When vision fails, the effects reach far beyond the eye itself.
Vision as an Enabler of Independence, Quality of Life, and Healthy Ageing
Independence represents one of the most valued outcomes of healthy ageing. Healthy-ageing frameworks consistently emphasise functional ability, autonomy, and the capacity to maintain independence throughout later life [37,62].
Vision plays a central role in achieving these goals. Daily activities such as reading medication labels, recognising hazards, preparing meals, managing finances, driving, navigating unfamiliar environments, and participating in social activities all depend upon adequate visual function.
When vision deteriorates, these activities may become increasingly difficult. Individuals may require greater support from family members, caregivers, or healthcare services. Over time, vision loss may contribute to reduced confidence, decreased mobility, social withdrawal, and loss of independence.
Vision directly shapes quality of life. The ability to read a book, recognise a loved one’s face, enjoy hobbies, engage in employment, participate in community activities, or safely manage daily tasks often depends upon maintaining functional vision.
Visual impairment has also been associated with:
– Increased risk of falls [10]
– Reduced mobility and impaired physical functioning [11]
– Depression and anxiety [8,9]
– Social isolation and reduced social participation [8,13,59]
– Reduced quality of life [13]
– Loss of independence and greater caregiver dependence [11,13]
Older adults with moderate to severe visual impairment may experience a significantly increased risk of falls compared with their peers, highlighting the broader implications of vision loss beyond ophthalmology alone [10,11].
From a healthy-ageing perspective, vision should therefore be viewed not solely as a clinical outcome but as a determinant of functional ability and wellbeing.
Lancet Global Health commentary has also highlighted ageing and vision loss as an emerging public-health priority. As populations live longer, preserving vision becomes essential to independence, participation, and quality of life throughout later life [63].
The Longevity–Vision Paradox
One of the defining challenges of modern ageing societies is the Longevity–Vision Paradox.
Advances in medicine, public health, and socioeconomic development have enabled people to live longer than at any point in human history.
The success of healthy-ageing policies therefore creates increasing demand for vision-preservation strategies. Longer lives represent a major achievement. However, longer lives must also be accompanied by efforts to preserve functional vision, independence, and quality of life. The importance of vision within healthy ageing is further strengthened by recent Lancet Commission analyses recognising vision impairment as a potentially modifiable risk factor for dementia. These observations reinforce the argument that vision preservation should be integrated into broader healthy-ageing, cognitive-health, and public-health strategies [60].
Without effective vision-preservation strategies, societies risk extending lifespan without fully preserving functional wellbeing. This paradox will become increasingly central as global populations continue to age.
Why Vision Should Be a Strategic Health-System Priority
Traditionally, vision care has often been viewed as a specialist clinical service. The Ageing Vision System suggests a broader perspective. Vision preservation should increasingly be recognised as a strategic objective for healthcare systems and ageing societies.
Several factors support this position.
Demographic Change – Population ageing will substantially increase demand for vision-care services, including AMD diagnosis, monitoring, treatment, rehabilitation, and long-term support.
Functional Independence – Vision preservation supports independent living and may reduce dependency on caregivers and support services.
Healthcare Utilisation – Visual impairment has been associated with falls-related injuries, reduced mobility, functional dependence, caregiver need, and long-term support requirements [10,11,13].
Economic Impact – The economic consequences of vision impairment extend far beyond healthcare expenditure alone. Global productivity losses associated with vision impairment have been estimated in the hundreds of billions of US dollars annually [1,7]. In addition, vision loss generates substantial indirect costs through reduced workforce participation, caregiver burden, social support requirements, and long-term care expenditure.
Social Participation – Preserving vision supports continued participation in family, community, cultural, and professional life.
Vision should be viewed not only as a clinical issue, but also as a public-health, economic, and societal priority.
A Patient Perspective
I think of Mrs. K as an anonymised composite of many patients: a retired teacher whose weekends once revolved around reading, preparing lunch for family, and recognising every face at the table. At first, the letters on the page only seemed distorted. Then faces across the room became uncertain. Later, unfamiliar pavements felt unsafe. Her measured visual acuity could still look deceptively reasonable, yet her world had already started to shrink. The cost to the healthcare system may be measurable. The cost to confidence and independence is harder to count.
That is the point. Preserving vision is not only about maintaining visual acuity. It is about preserving autonomy.
A Global Perspective
The implications of vision loss extend beyond high-income countries. In many low- and middle-income countries, access to eye care, retinal services, rehabilitation programmes, assistive technologies, and social support systems remains limited. In these settings, visual impairment may affect employment, education, family wellbeing, economic participation, and social inclusion. For many individuals, vision preservation is not merely a quality-of-life issue. It is a determinant of economic security, equity, and opportunity. Healthy-ageing strategies must therefore address avoidable vision loss and strengthen access to vision care globally.
Implications for AMD
AMD provides one of the clearest examples of why The Ageing Vision System matters. The burden of AMD is closely linked to demographic ageing. As populations grow older, AMD will become increasingly central to healthcare systems, policymakers, and societies. The challenge therefore extends beyond treating retinal disease. It involves preserving the functional abilities that allow individuals to remain independent, socially engaged, economically active, and connected to their communities throughout later life. The broader view provides the foundation for understanding AMD not simply as an ophthalmic condition, but as a challenge of healthy ageing itself.
Conclusion
Contemporary healthy-ageing research increasingly recognises that successful longevity requires preservation of multiple domains of function rather than survival alone. Recent work published in Nature Medicine similarly emphasises the maintenance of cognitive, physical, and mental health alongside freedom from major chronic disease as key components of healthy ageing, supporting a broader multidimensional understanding of ageing well [62].
The Ageing Vision System offers a simple shift in perspective. Vision should no longer be viewed only as a sensory function managed within specialist ophthalmic services. It is a core determinant of healthy ageing, independence, wellbeing, and quality of life. As populations age, preserving vision becomes a strategic objective for individuals, healthcare systems, and societies. The next question is how care systems can protect that vision at scale.
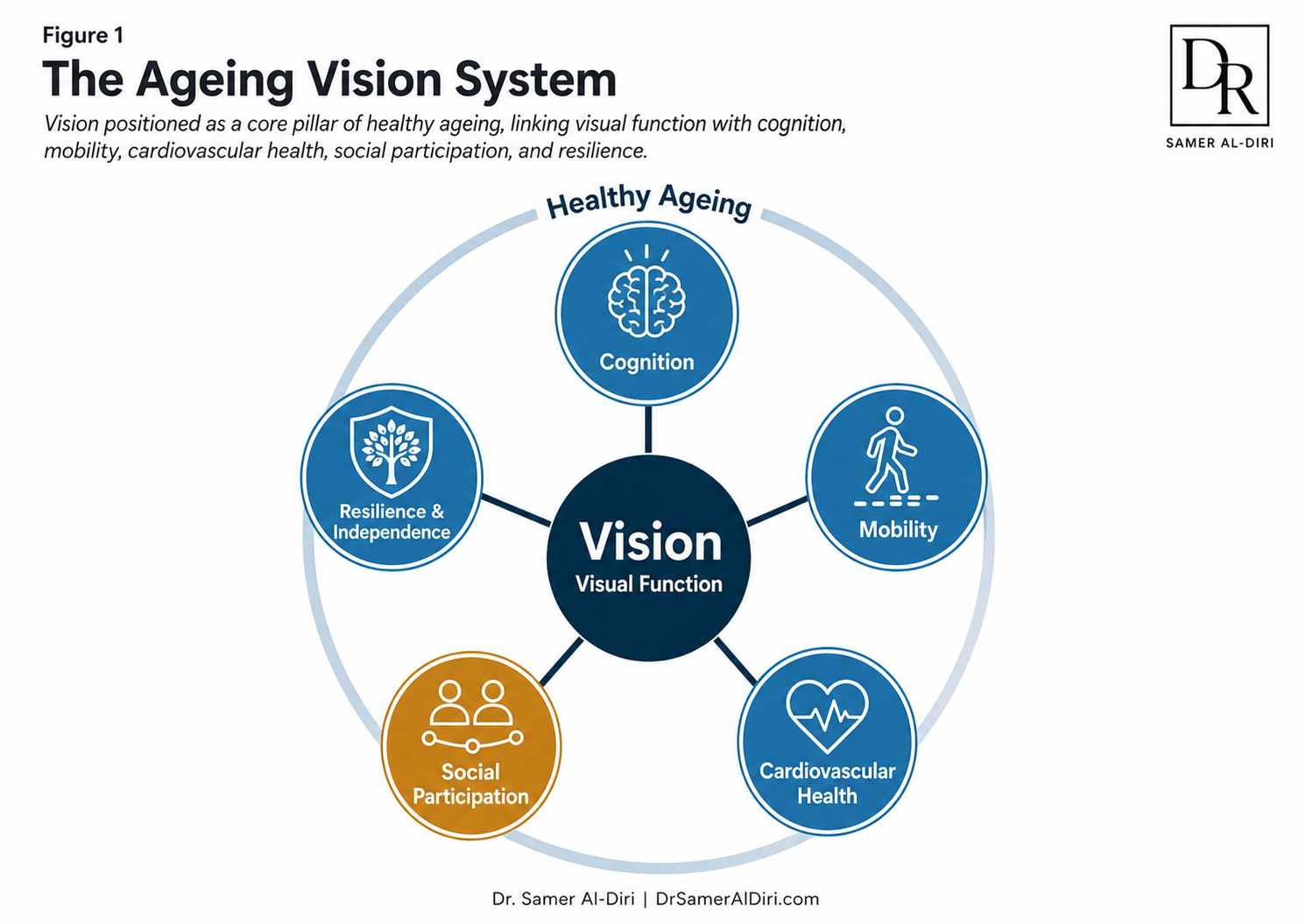
Figure 1. The Ageing Vision System: vision positioned as a core pillar of healthy ageing, linking visual function with cognition, mobility, cardiovascular health, social participation, and resilience.
The Sustainable Vision Care Framework
Building Future-Ready Vision-Care Systems for Ageing Societies
Introduction
The future challenge of age-related macular degeneration (AMD) extends beyond scientific discovery. The development of new therapies, advances in retinal imaging, progress in artificial intelligence, and innovations in regenerative medicine represent major achievements in ophthalmology. However, innovation alone will not determine future outcomes.
The central question facing ageing societies is no longer simply whether better treatments can be developed. The more critical question is whether healthcare systems can deliver effective, equitable, accessible, and sustainable vision care to growing populations at risk of visual impairment.
Sustainable vision care begins with a practical question: how can future vision-care systems preserve functional vision, independence, wellbeing, and quality of life across longer lifespans?
The argument aligns closely with the World Health Organization’s emphasis on integrated people-centred eye care and with growing recognition that vision health is a fundamental component of healthy ageing, social participation, and human capital development [1,38,40].
This approach also aligns with recommendations from the Lancet Global Health Commission on Global Eye Health, which emphasised integrated, equitable, people-centred eye-care systems capable of responding to population ageing, increasing demand, and persistent inequalities in access to care [59].
Sustainable vision care therefore requires coordinated action across prevention, early detection, treatment, rehabilitation, workforce development, technological innovation, implementation science, and health-system planning.
Why Existing Vision-Care Models May No Longer Be Sufficient
Many contemporary eye-care systems were developed during an era characterised by shorter life expectancy, lower prevalence of chronic age-related disease, limited therapeutic options, lower imaging volumes, and less intensive monitoring requirements. The landscape has changed fundamentally. Ageing populations, chronic disease growth, increasing patient expectations, emerging therapies, artificial intelligence, and expanding diagnostic capabilities are transforming demand for vision-care services.
At the same time, many healthcare systems face workforce shortages, financial constraints, geographic inequities, increasing service complexity, and growing implementation challenges. Traditional service models may therefore struggle to meet future demand. The challenge is not simply delivering more care. The challenge is delivering sustainable care.
Why Sustainability Matters in Vision Care
Sustainability should not be interpreted as cost containment alone. Rather, sustainable vision care refers to the ability of healthcare systems to continue delivering high-quality, equitable, and effective services while adapting to demographic, technological, and epidemiological change.
Healthcare systems that focus solely on short-term efficiency may struggle to respond to future demand. Conversely, systems that invest in prevention, workforce development, innovation, and resilience are more likely to remain effective over time. Sustainable vision care therefore represents a strategic rather than purely operational objective.
The Six Pillars of The Sustainable Vision Care Framework
Six interconnected pillars support future-ready vision-care systems.
Pillar 1: Prevention and Risk Reduction – The most sustainable vision loss is vision loss that never occurs. Although AMD cannot always be prevented, opportunities exist to reduce risk and delay progression through smoking cessation, cardiovascular risk-factor control, healthy nutrition, AREDS2-informed advice where clinically appropriate, public awareness initiatives, and earlier engagement with eye-care services [36].
Pillar 2: Early Detection and Timely Diagnosis – Many retinal diseases become increasingly difficult to manage when diagnosed late. Early detection creates opportunities for earlier intervention, better patient education, improved monitoring, rehabilitation planning, and risk stratification. Future systems should increasingly utilise community-based detection programmes, digital referral pathways, teleophthalmology, AI-assisted screening, and risk-based surveillance strategies.
Pillar 3: Effective and Equitable Treatment – Scientific innovation remains central to future vision care. However, innovation alone is insufficient. The true value of innovation depends upon implementation. Treatments must be accessible, affordable, equitably distributed, and operationally deliverable. A therapy that exists but remains inaccessible to large populations cannot achieve its full public-health potential.
Pillar 4: Rehabilitation and Functional Support – Vision care should not end when treatment options are exhausted. Low-vision support, assistive technologies, orientation and mobility training, occupational and psychological support, and social support services help preserve independence, dignity, and participation. Rehabilitation is an essential component of sustainable care.
Pillar 5: Workforce and System Capacity – The greatest future limitation in vision care may not be scientific innovation but workforce capacity. Growing demand for retinal imaging, intravitreal therapy, chronic disease monitoring, Geographic Atrophy management, and long-term follow-up is creating substantial pressure on healthcare systems worldwide. Future success depends on workforce planning, training and retention, expanded multidisciplinary care, service redesign, appropriate task sharing, and strategic use of technology.
Pillar 6: Technology, Artificial Intelligence, and Health-System Innovation – Artificial intelligence, advanced imaging, predictive analytics, teleophthalmology, remote monitoring, and digital health platforms may help improve efficiency, access, and personalisation of care. However, technology should be viewed as an enabler rather than an objective. The goal is better patient outcomes, more efficient services, improved access, and stronger health-system resilience.

Figure 2. The Sustainable Vision Care Framework: six pillars for a future-ready vision-care ecosystem across prevention, early detection, optimal treatment, rehabilitation, workforce capacity, and technology and data innovation.
The Economic Case for Sustainable Vision Care
Vision impairment imposes substantial costs on individuals, families, healthcare systems, and economies, including direct healthcare expenditure, long-term social-care costs, caregiver burden, productivity losses, reduced workforce participation, and loss of independence [7,39,40]. Global productivity losses associated with vision impairment have been estimated in the hundreds of billions of US dollars annually [7]. Conversely, investments in prevention, timely intervention, and vision preservation may generate substantial social and economic returns. Sustainable vision care should therefore be viewed not only as a healthcare priority but also as an economic and societal investment.
The Vision Dividend
Preserving vision generates benefits that extend far beyond the eye. When individuals retain functional vision for longer, society gains a Vision Dividend: a measurable return on investment in prevention, early detection, treatment, rehabilitation, and sustainable eye-care services.
The Vision Dividend includes:
– Health gains – fewer falls, injuries, and hospital admissions; better management of chronic diseases; preserved mental wellbeing and cognition.
– Social gains – maintained independence, social participation, driving, reading, and caregiving capacity for families.
– Economic gains – reduced long-term care costs, higher workforce participation among older adults, lower productivity losses, and delayed entry into residential care.
– Health-system gains – more efficient use of specialist workforces, fewer unnecessary clinic visits, and reduced pressure on emergency and social services.
In ageing societies, the Vision Dividend transforms vision preservation from a healthcare cost into a strategic investment in human capital, healthy longevity, and fiscal sustainability. The Vision Dividend therefore aligns vision care with broader societal goals of healthy longevity, economic productivity, and sustainable health-system development.
For AMD, investment in timely detection, effective treatment, and vision rehabilitation may generate downstream savings while helping preserve independence.
This reframing reinforces the central message of The Sustainable Vision Care Framework: future-ready systems must be designed not merely to treat retinal disease, but to protect the capabilities – reading, mobility, confidence, connection – that functional vision makes possible.
A Patient Perspective
Consider Mr. A, a 74-year-old retired engineer diagnosed with intermediate AMD. Within a sustainable vision-care system, he receives early diagnosis, education regarding risk reduction, regular monitoring, timely referral when disease progression occurs, access to treatment when appropriate, and rehabilitation support if visual impairment develops. As a result, he remains independent, socially engaged, and able to continue participating in daily life. The goal is not simply to treat disease. The goal is to preserve lives lived well.
A Global Perspective
The need for sustainable vision care extends far beyond high-income countries. Many low- and middle-income countries face substantial unmet eye-care needs, workforce shortages, infrastructure limitations, and geographic barriers to access. At the same time, these countries are experiencing rapid demographic transitions and increasing prevalence of chronic diseases. The Sustainable Vision Care Framework is therefore intended to be adaptable rather than prescriptive. The principles remain constant; implementation must reflect local realities.
Sustainable Vision Care and Health-System Resilience
Future-ready vision-care systems must be capable of adapting to population ageing, workforce pressures, technological transformation, therapeutic innovation, and economic constraints. This adaptive capacity may be described as Vision-System Resilience. Resilient systems are more likely to translate scientific advances into meaningful patient benefit. Less resilient systems risk widening inequities, increasing delays, and creating implementation bottlenecks.
Implications for AMD
AMD provides one of the clearest examples of why sustainable vision care matters. The future burden of AMD will be shaped not only by disease prevalence but also by demographic ageing, workforce capacity, artificial intelligence, health-system preparedness, healthcare financing, and implementation capability. Successfully managing AMD therefore requires systems capable of delivering prevention, diagnosis, treatment, rehabilitation, monitoring, and long-term support at population scale.
Conclusion
The future of vision care will not be determined solely by scientific breakthroughs. It will be determined by whether healthcare systems can successfully translate innovation into equitable, accessible, and sustainable patient benefit. The Sustainable Vision Care Framework provides an analytical lens for integrating prevention, early detection, treatment, rehabilitation, workforce development, technology, implementation, and health-system resilience into a coordinated strategy. As populations continue to age, sustainable vision care is not simply an ophthalmic objective – it is a healthy-ageing, health-system, and societal objective.
AMD and the Global Burden of Population Ageing
Epidemiology, Demographic Change, and the Future Burden of Vision Loss
Introduction
Age-related macular degeneration (AMD) is one of the leading causes of irreversible visual impairment and blindness worldwide and represents a growing challenge for ageing societies. While AMD has long been recognised as an important retinal disease, demographic transformation is changing both its scale and significance.
The future burden of AMD will be shaped not only by biological risk factors and therapeutic innovation, but also by one of the most powerful forces in modern healthcare: population ageing. As life expectancy increases and populations grow older, the number of individuals at risk of AMD continues to rise. AMD is now a public-health challenge, a healthy-ageing challenge, and a health-system challenge.
Understanding the future of AMD therefore requires an understanding of demographic change itself.
AMD in a Global Context
AMD affects millions of people worldwide and remains among the leading causes of irreversible visual impairment in older adults. A landmark global analysis estimated that approximately 196 million people were living with AMD in 2020, with projections suggesting that this number could increase to nearly 290 million by 2040 if demographic trends continue [2].
Of these individuals, more than five million are estimated to be affected by Geographic Atrophy (GA), the advanced atrophic form of AMD and a major cause of irreversible central vision loss in older adults [64]. Because GA is strongly age-dependent, its prevalence is expected to increase disproportionately as populations continue to age. GA may therefore grow even more rapidly than AMD overall, creating additional challenges for patients, healthcare systems, and society.
These estimates highlight a central reality: the future burden of AMD is not static – it is expanding. More recent analyses from the Global Burden of Disease (GBD) programme and the Vision Loss Expert Group have reinforced this trajectory. AMD remains a leading cause of moderate-to-severe visual impairment and blindness among older adults across all world regions, reflecting the combined effects of demographic ageing, increasing longevity, and expanding populations at risk [4,41,61].
Recent analyses published in Lancet Global Health further demonstrate that AMD-related vision impairment continues to contribute substantially to the global burden of visual disability and that demographic ageing is expected to remain the principal driver of future AMD burden through 2050 [61].
Much of this increase is driven not by changes in disease biology, but by changes in population structure. As societies age, more people survive into the decades of life in which AMD becomes most prevalent. That demographic shift underpins much of the future challenge facing healthcare systems.
The Epidemiology of Ageing
Population ageing represents one of the most significant demographic transformations in human history. According to United Nations projections, the number of people aged 65 years and older is expected to increase dramatically over coming decades [5]. By 2050:
– One in six people globally will be aged 65 years or older.
– The number of adults aged 80 years and older is expected to approximately triple.
– Older populations will account for an increasingly large proportion of healthcare utilisation.
These trends are particularly relevant to AMD because age remains the strongest known risk factor for disease development. The prevalence of AMD rises sharply with advancing age. Population-based European analyses suggest that the prevalence of late AMD increases from approximately 0.1% among individuals aged 55–59 years to nearly 9.8% among those aged 85 years and older [65].
This steep age gradient explains why demographic ageing exerts such a powerful influence on future disease burden.
The Longevity–Vision Paradox Revisited
The Ageing Vision System is closely linked to the concept of the Longevity–Vision Paradox. The epidemiology of AMD provides one of the clearest illustrations of this phenomenon. Medical progress has successfully extended lifespan. However, longer lives increase cumulative exposure to age-related diseases. The result is a paradox: the same societal achievements that enable longer lives also increase demand for vision-preservation strategies.
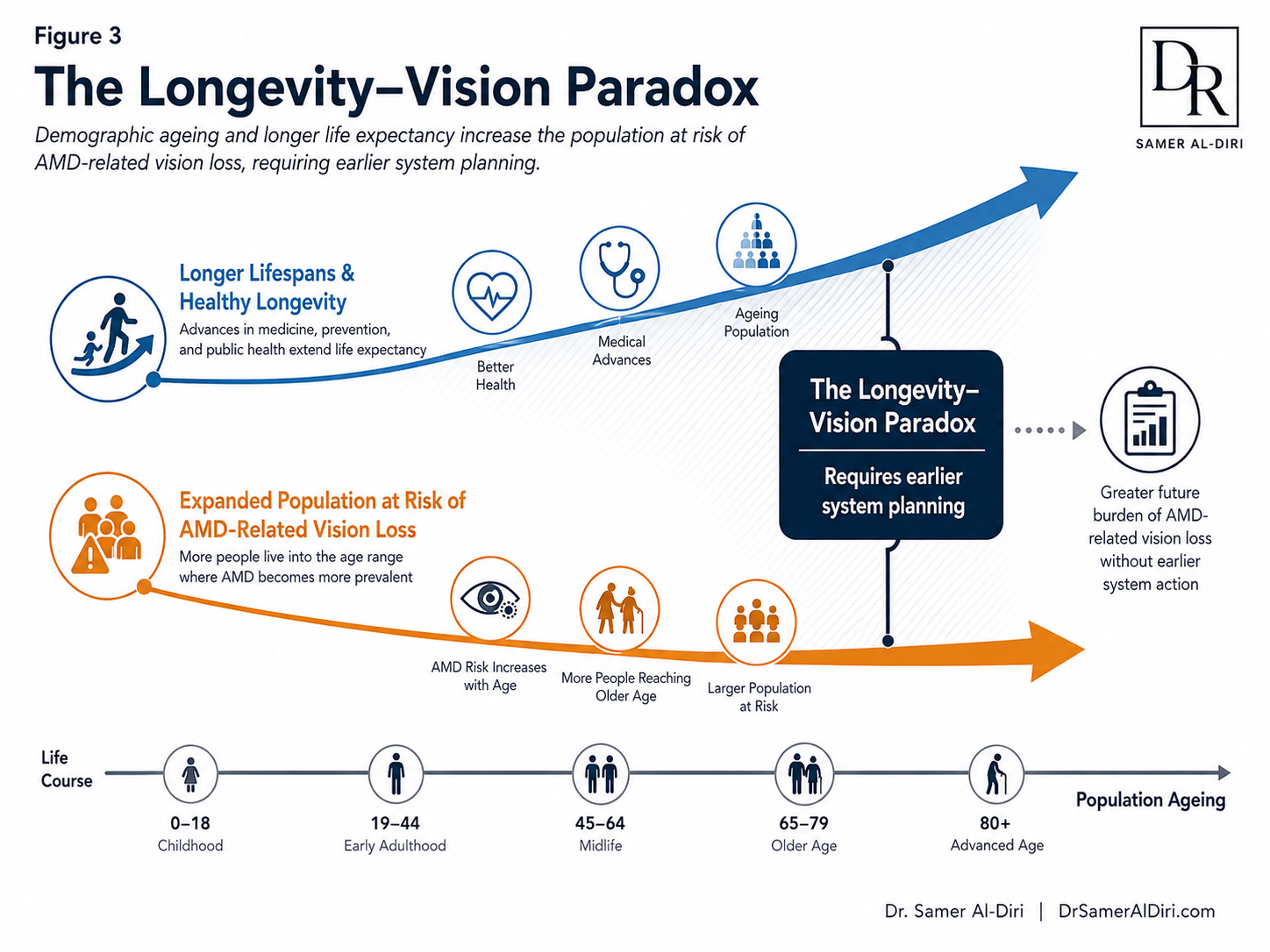
Figure 3. The Longevity–Vision Paradox: demographic ageing and longer life expectancy increase the population at risk of AMD-related vision loss, requiring earlier system planning.
AMD therefore represents one of the clearest examples of how demographic success generates new healthcare challenges. Future health systems must prepare not only for increased longevity but also for the consequences of longer lives.
Geographic Variation and Global Inequities
The burden of AMD is not distributed equally. Significant geographic variation exists across regions, populations, and healthcare systems. High-income countries often report greater AMD prevalence, partly because of longer life expectancy and more comprehensive diagnostic services. However, lower- and middle-income countries are experiencing rapid demographic transitions and may face substantial future increases in AMD burden.
Several factors influence regional variation: population age structure, life expectancy, access to eye-care services, diagnostic capacity, public awareness, health literacy, and socioeconomic conditions. Many health systems undergoing the fastest demographic transitions also have limited retina-care infrastructure, workforce capacity, and access to advanced therapies. Future AMD care could therefore widen inequities unless access is planned deliberately.
Beyond Prevalence: The True Burden of AMD
Epidemiological statistics capture only part of the AMD story. The true burden extends beyond prevalence and incidence. AMD may influence independence, reading ability, face recognition, mobility, social participation, mental wellbeing, quality of life, and caregiver burden. The societal burden of AMD extends far beyond visual impairment alone. From a public-health perspective, AMD should increasingly be viewed as a condition that affects functional ageing rather than simply visual function.
Patient Perspective – For an 80-year-old individual living with AMD, the burden of disease cannot be fully expressed through prevalence statistics, risk ratios, or epidemiological projections. The true stakes may be the ability to continue reading independently, recognising family members, maintaining mobility, participating in community life, or remaining in one’s own home. For patients, the consequences of AMD are measured not only in visual outcomes but also in the preservation of independence, identity, and dignity.
The Economic Burden of AMD
AMD is expensive – not only in medications, clinic visits, imaging, treatments, and rehabilitation. The costs also appear in lost productivity, informal caregiving, transport, reduced workforce participation, and long-term support. Global productivity losses attributable to vision impairment and blindness have been estimated at more than US$400 billion annually [7]. These estimates likely underestimate the true societal burden because they do not fully capture family time, social withdrawal, diminished quality of life, and the long-term consequences of lost independence. As populations age, these costs will grow. The future challenge of AMD is therefore not solely clinical — it is economic and deeply human.
AMD as a Public-Health Challenge
Several characteristics distinguish AMD as a major public-health issue: scale, demographic growth, functional impact, service demand, and equity. Millions are affected worldwide. The population at risk continues to grow. AMD affects independence, healthy ageing, and quality of life, while access to diagnosis, treatment, rehabilitation, and emerging therapies remains uneven. These features make AMD an urgent public-health priority for ageing societies.
Implications for Health Systems
The pressure is already visible in many services. More patients need imaging, monitoring, injections, rehabilitation, and long-term follow-up. Add GA therapies to this landscape and the question becomes unavoidable: can systems expand fast enough without compromising equity or quality?
Looking Ahead
The epidemiology of AMD tells a broader story than disease prevalence alone. It tells the story of ageing societies. The increasing burden of AMD reflects profound demographic changes that are reshaping healthcare systems worldwide. As populations continue to age, preserving vision will become increasingly central to maintaining independence, wellbeing, social participation, and healthy ageing. AMD therefore serves as an indicator of how successfully societies respond to the challenges of demographic change.
Conclusion
AMD is emerging as one of the defining vision-health challenges of the twenty-first century. Population ageing, increasing life expectancy, and expanding demand for vision care will increase the future burden of disease. The issue extends beyond ophthalmology into public health, healthy ageing, healthcare management, workforce planning, health economics, and health-system sustainability. Epidemiology explains why the task is urgent. The next section turns from populations to people.
The Human Impact of Age-Related Macular Degeneration
Age-related macular degeneration (AMD) is often described through OCT scans, lesion classification, visual acuity, and treatment outcomes. These measures matter. But they do not fully capture what the disease does to a life. For many patients, AMD is experienced less as a retinal diagnosis and more as the slow loss of confidence, routine, identity, and independence.
The consequences of AMD extend far beyond visual impairment. The disease influences how people read, recognise faces, navigate unfamiliar environments, drive, manage medications, participate in social activities, and maintain their independence. As populations age and life expectancy continues to increase globally, understanding the human impact of AMD becomes increasingly central for clinicians, policymakers, health-system leaders, and society as a whole.
The human consequences of AMD are easiest to understand through lived experience. Mrs. S is an anonymised composite, but her story is familiar in retina clinics. She is a 78-year-old retired schoolteacher with intermediate AMD and visual acuity around 20/40. On paper, that can look “not too bad.” In life, it can be devastating. She no longer reads novels for pleasure because the words blur and break. She hesitates when greeting people across a room because she is no longer sure who they are. She stops driving, not after an accident, but after losing confidence on unfamiliar roads. Clinically, her disease may appear moderate. Functionally, her world has become much smaller.
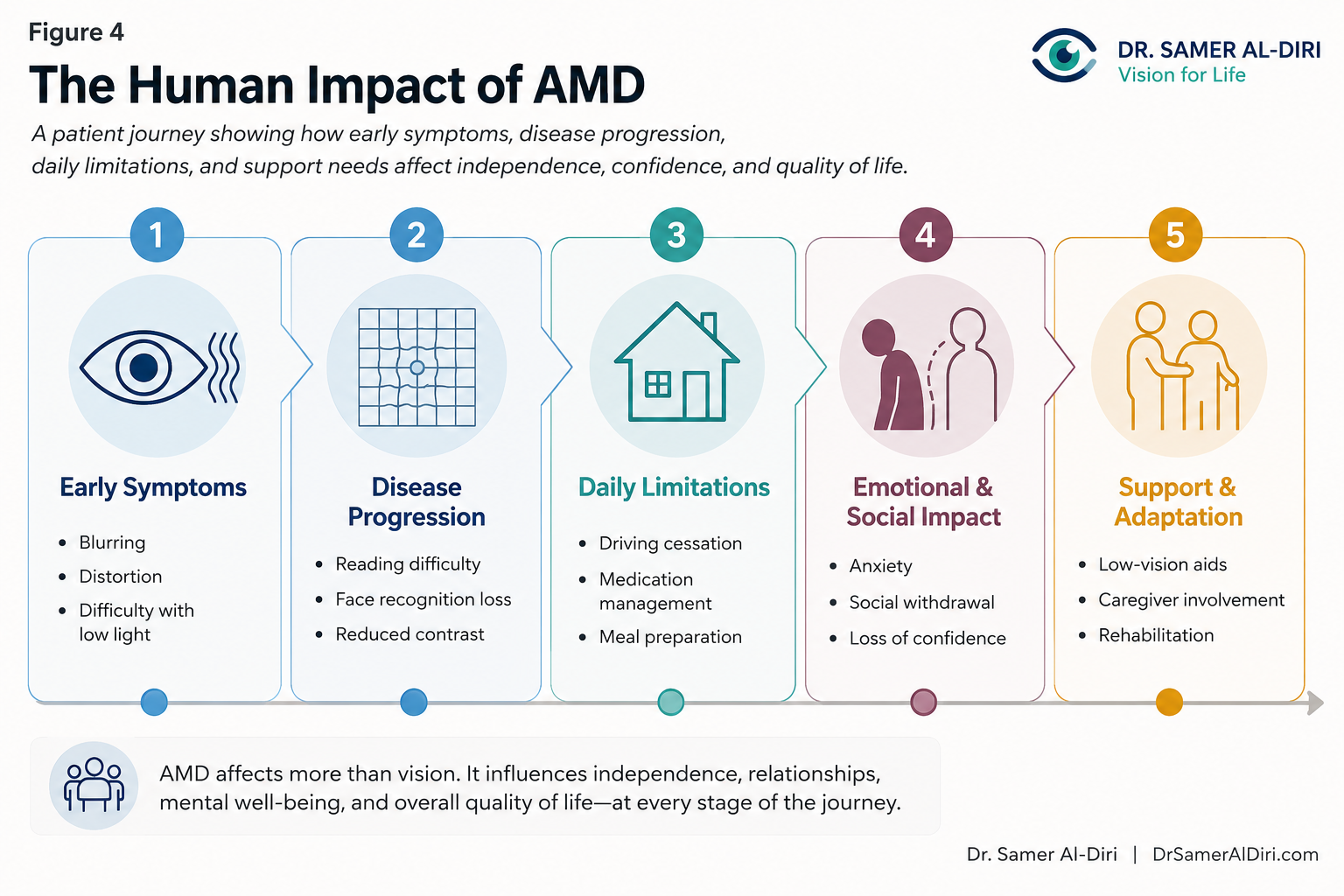
Figure 4. The Human Impact of AMD: a patient journey showing how early symptoms, disease progression, daily limitations, emotional and social impact, and support needs affect independence, confidence, and quality of life.
This is a simplified clinical map rather than a full psychosocial model; its purpose is to keep patient experience visible alongside anatomy, treatment decisions, and system design.
Her experience illustrates a central reality: the burden of AMD cannot be understood through retinal imaging or visual acuity measurements alone.
Lessons from the Clinic
What has struck me most in clinical practice is how differently patients respond to the same measured vision. One person with 20/80 adapts, uses low-vision aids, and keeps reading. Another with 20/40 feels that life has been sharply interrupted. We are not treating maculae alone. We are treating expectations, habits, families, fear, and resilience.
Vision Loss and the Erosion of Everyday Independence
Central vision plays a critical role in many activities that individuals often take for granted. Reading correspondence, viewing digital devices, identifying medication labels, preparing meals, recognising family members, managing finances, and driving all depend heavily on intact macular function. As AMD progresses, these activities can become increasingly difficult or impossible.
Patients frequently describe a gradual narrowing of their functional world. Tasks that once required little effort may become frustrating, time-consuming, or unsafe. Reading speed declines, facial recognition becomes unreliable, and confidence in performing routine activities diminishes. For many older adults, the loss of driving privileges represents a particularly painful turning point, often reducing mobility, limiting social engagement, and increasing dependence on others.
Visual acuity alone does not capture the impact of AMD. Two individuals with similar clinical findings may experience very different levels of functional impairment depending on lifestyle, support systems, occupational demands, psychological resilience, and environment. Patient-centred assessment must therefore look beyond ophthalmic measurements to quality of life, functional status, patient-reported impact, and individual goals [42,64].
The Psychological and Emotional Burden of AMD
The emotional consequences of AMD are substantial and increasingly recognised within the scientific literature. Visual impairment can threaten an individual’s sense of autonomy, competence, and self-identity. Patients may experience frustration, anxiety, fear regarding future vision loss, and uncertainty about disease progression.
Systematic reviews and observational studies suggest that clinically significant depressive symptoms may affect up to one-third of individuals living with AMD, a prevalence substantially higher than that observed among age-matched individuals without visual impairment [8,9]. Anxiety regarding future vision loss, uncertainty about disease progression, and concerns regarding loss of independence frequently contribute to psychological distress. The inability to read, pursue hobbies, recognise faces, or participate fully in social interactions may further intensify feelings of isolation and loss of purpose.
These findings reinforce a practical principle: emotional wellbeing should be regarded as a core outcome of AMD care rather than merely a secondary consequence of disease. Effective management requires recognition of the psychological, social, and emotional dimensions of vision loss alongside medical treatment.
Social Isolation and the Loss of Human Connection
Vision plays a central role in communication and social participation. Facial recognition, interpretation of non-verbal cues, and participation in shared activities are all influenced by visual function. As AMD progresses, social interactions may become increasingly challenging.
Individuals with visual impairment may avoid social gatherings because of difficulty recognising people, navigating unfamiliar environments, or participating in group activities. Over time, this can contribute to reduced social engagement and increased isolation. Such isolation is itself associated with poorer mental health, reduced physical activity, diminished wellbeing, and increased vulnerability among older adults.
The effects extend beyond the individual patient. Family members and friends may struggle to appreciate the extent of functional impairment, particularly during earlier stages of disease when vision loss may not be outwardly obvious. This mismatch between clinical appearance and lived experience can create additional emotional challenges for patients attempting to adapt to progressive visual decline.
Falls, Frailty, and Physical Health Consequences
The consequences of AMD extend beyond vision and mental health to include important physical health risks. Visual impairment, reduced contrast sensitivity, and optical factors affecting hazard detection are associated with an increased likelihood of falls, injuries, fractures, and loss of mobility [6,10,11]. These risks are particularly significant among older adults, many of whom may already be living with frailty, multimorbidity, or reduced physiological reserve.
Research suggests that older adults with moderate-to-severe visual impairment experience approximately 1.5- to 2-fold higher risks of falls compared with individuals with normal vision [10,11]. Falls may trigger a cascade of adverse outcomes, including hospitalisation, prolonged rehabilitation, disability, institutionalisation, and substantial loss of independence. In many cases, the downstream consequences of a serious fall may ultimately have a greater impact on quality of life than the visual impairment itself.
The relationship between AMD and falls highlights a broader reality: visual health and overall health are inseparable. Preserving vision is therefore not solely an ophthalmic objective but a central component of healthy ageing, mobility, safety, and functional independence.
The Importance of Low-Vision Rehabilitation
Many of the functional consequences of AMD are not inevitable. Low-vision rehabilitation services can help individuals adapt to visual impairment and maintain independence despite disease progression. Such interventions may include magnification devices, enhanced lighting strategies, electronic reading aids, orientation and mobility training, home-safety assessments, occupational therapy support, digital assistive technologies, and environmental modifications. Evidence suggests that low-vision rehabilitation can improve functional performance, confidence, and quality of life for many individuals living with AMD [12].
Despite these benefits, access to rehabilitation services remains highly variable across healthcare systems. In many countries, low-vision services remain underfunded, underdeveloped, or insufficiently integrated into routine ophthalmic care. As populations age and AMD prevalence increases, strengthening rehabilitation capacity should become an integral component of sustainable vision-care planning.
The Hidden Burden on Families and Caregivers
AMD affects not only patients but also families, caregivers, and support networks. As visual impairment progresses, many individuals require assistance with transportation, medication management, household tasks, shopping, financial administration, and attendance at medical appointments.
Studies suggest that caregivers of individuals with advanced AMD may spend approximately 10–20 hours per week providing support, often while balancing employment, family responsibilities, and their own health needs [13]. Many caregivers report substantial emotional strain, disruption of employment, reduced social participation, and financial pressures associated with caregiving responsibilities.
Caregiver strain is a central but often overlooked part of AMD’s societal impact. The consequences extend beyond healthcare expenditure and clinic visits to countless hours of unpaid care provided by relatives and loved ones. Direct medical costs capture only part of the burden.
AMD and the Longevity–Vision Paradox
The growing human burden of AMD reflects a broader demographic reality that may be described as the Longevity–Vision Paradox. Advances in medicine, public health, and socioeconomic development have enabled people to live longer than at any previous point in human history. Yet increasing longevity simultaneously expands the population at risk of age-related visual disorders. One of humanity’s greatest achievements – longer life expectancy – therefore creates new challenges for maintaining vision, independence, and quality of life in later life.
This paradox highlights why AMD should be viewed not merely as a retinal disease but as a defining challenge of ageing societies. The future burden of AMD will depend not only on scientific advances in treatment but also on the ability of health systems to support healthy ageing, equitable access to care, rehabilitation services, and long-term vision preservation.
Reframing AMD Through The Ageing Vision System
The human consequences of AMD reinforce the central concept of The Ageing Vision System. Vision in later life is shaped by a complex interaction between biological ageing, chronic disease, healthcare access, social support, technological innovation, rehabilitation capacity, and health-system resilience. AMD represents more than degeneration of the macula – it is a condition that influences independence, mental health, social participation, physical wellbeing, caregiver burden, and societal resilience. The ultimate goal of AMD management should be to preserve functional vision, maintain independence, support psychological wellbeing, reduce avoidable disability, and enable individuals to continue living meaningful and connected lives.
From Anatomical Outcomes to Meaningful Human Outcomes
The distinction between clinical outcomes and lived experience is increasingly central in contemporary AMD care. Advances in imaging technologies and emerging therapies have improved the ability to measure disease progression and modify anatomical outcomes. However, patients, clinicians, and policymakers are ultimately concerned with outcomes that matter in everyday life: reading ability, mobility, independence, confidence, social participation, and quality of life.
Nowhere is this more relevant than in Geographic Atrophy. Emerging therapies can slow anatomical lesion growth, which is a genuine scientific achievement. Yet the central question remains whether structural benefit becomes meaningful functional benefit for patients. In clinical practice, the distance between a stable scan and a reassured patient can be surprisingly wide. Patients rarely ask about square millimetres of atrophy; they ask whether they will keep reading, driving, or recognising the people they love. Preserving retinal tissue matters because it may help preserve a life lived with independence and dignity.
Key Message
The greatest burden of age-related macular degeneration is not measured solely in retinal scans, clinic visits, or visual acuity charts. It is measured in lost independence, diminished confidence, reduced social participation, caregiver strain, increased vulnerability, and impaired quality of life. That human burden leads directly to the next question: can health systems respond at the scale required?
Health-System Impact of Age-Related Macular Degeneration
Service Demand, Resource Utilisation, and the Challenge of Sustainable Care
Age-related macular degeneration (AMD) is often discussed in terms of retinal pathology, disease progression, and therapeutic innovation. However, at a population level, AMD represents far more than a clinical condition. It is increasingly a health-system challenge that influences workforce requirements, service demand, infrastructure capacity, healthcare expenditure, and long-term sustainability.
The growing number of individuals living with AMD is generating rising demand for ophthalmic services, retinal imaging, specialist consultations, monitoring programmes, rehabilitation services, and long-term support systems. As populations age worldwide, health systems must prepare not only for more patients with AMD, but also for substantially greater complexity in service delivery.
In many healthcare systems, ophthalmology has become one of the busiest outpatient specialties. NHS England reports more than eight million ophthalmology outpatient appointments annually, reflecting the growing burden of chronic eye disease and ageing populations [14]. Similar trends are observed across many high-income countries, where increasing longevity and improved survival from chronic disease are contributing to unprecedented demand for eye-care services and workforce-capacity planning [44].
The challenge is therefore no longer simply how to diagnose and treat AMD. The challenge is whether health systems can provide timely, equitable, and sustainable care at the scale required by ageing populations.
The Expanding Imaging Burden
Modern AMD management depends heavily on imaging. Optical Coherence Tomography (OCT) has transformed retinal care by enabling high-resolution visualisation of retinal anatomy, facilitating earlier diagnosis, treatment monitoring, and disease stratification. However, this clinical success has created an expanding imaging burden. A single high-volume retinal clinic may perform hundreds of OCT scans each week, while major tertiary centres may perform many thousands annually. Every scan requires specialised equipment, trained personnel, image interpretation, documentation, quality assurance, and integration into clinical decision-making pathways.
The future burden of AMD is therefore not only a patient burden. It is also an imaging and data-management burden. Rising OCT and retinal-imaging volumes create new demands for digital infrastructure, image storage, workflow optimisation, and clinical governance. Artificial intelligence may help through automated image analysis, triage, risk prediction, and workflow prioritisation. Even so, safe implementation still requires well-designed governance, validation, workforce training, and regulatory oversight. AMD care will depend not only on clinical expertise, but also on the ability of health systems to manage growing imaging data efficiently and safely.
The Injection Burden
The introduction of anti-vascular endothelial growth factor (anti-VEGF) therapies transformed the management of neovascular AMD and remains one of modern ophthalmology’s great therapeutic successes. More durable nAMD strategies, including faricimab extended-interval dosing, aflibercept 8 mg, home OCT-guided monitoring, and the Port Delivery System with ranibizumab, show how the field continues to reduce treatment burden while preserving disease control [31–35]. Yet success created volume. In England, Public Health England reported 608,000 intravitreal injection procedures during 2019/20 among people aged 60 years and older — roughly twelve thousand procedures each week [15]. On paper, that is a service statistic. In clinic, it means full waiting rooms, injection lists running late, and patients arranging transport for a procedure that may take minutes but shape the rest of their month.
I have seen clinics where injection lists run late into the evening. That is what therapeutic success can look like from the inside: better outcomes, but real pressure on patients, staff, and clinic systems.
Each injection requires clinic space, trained clinicians, nursing support, consumables, imaging resources, administrative capacity, and follow-up. The practical lesson is clear: therapeutic innovation may improve outcomes while increasing workload. Success in chronic retinal disease often generates more demand, not less. AMD therefore shows why scientific progress must be matched by workforce planning and service redesign.
AMD and the Challenge of Long-Term Monitoring
Unlike many acute conditions, AMD frequently requires prolonged engagement with healthcare services. Patients may require years of monitoring, repeated imaging, serial treatments, rehabilitation support, and ongoing reassessment. As life expectancy increases, many individuals will live with AMD for extended periods, generating cumulative service demand across decades rather than months. This long-term nature of care creates sustained pressure on outpatient clinics, imaging facilities, treatment centres, and specialist workforces. Health systems designed around episodic care may struggle to accommodate conditions that require continuous surveillance and management.
Geographic Atrophy: The Next Capacity Multiplier
The emergence of disease-modifying therapies for Geographic Atrophy (GA) is one of the central developments in contemporary retinal medicine. For the first time, therapeutic options are becoming available for a condition once managed mainly through observation and supportive care. Scientific progress, however, creates new implementation pressures. Disease-modifying therapies may require regular clinic attendance, imaging, treatment delivery, and long-term monitoring. Even modest uptake among eligible patients could increase clinic activity, imaging volumes, workforce demand, and healthcare expenditure. GA is therefore both a therapeutic challenge and a capacity challenge. Breakthroughs matter most when health systems can deliver them.
(A more comprehensive discussion of GA therapeutics, including trial data, safety, and the functional-structural debate, is provided in the following chapters.)
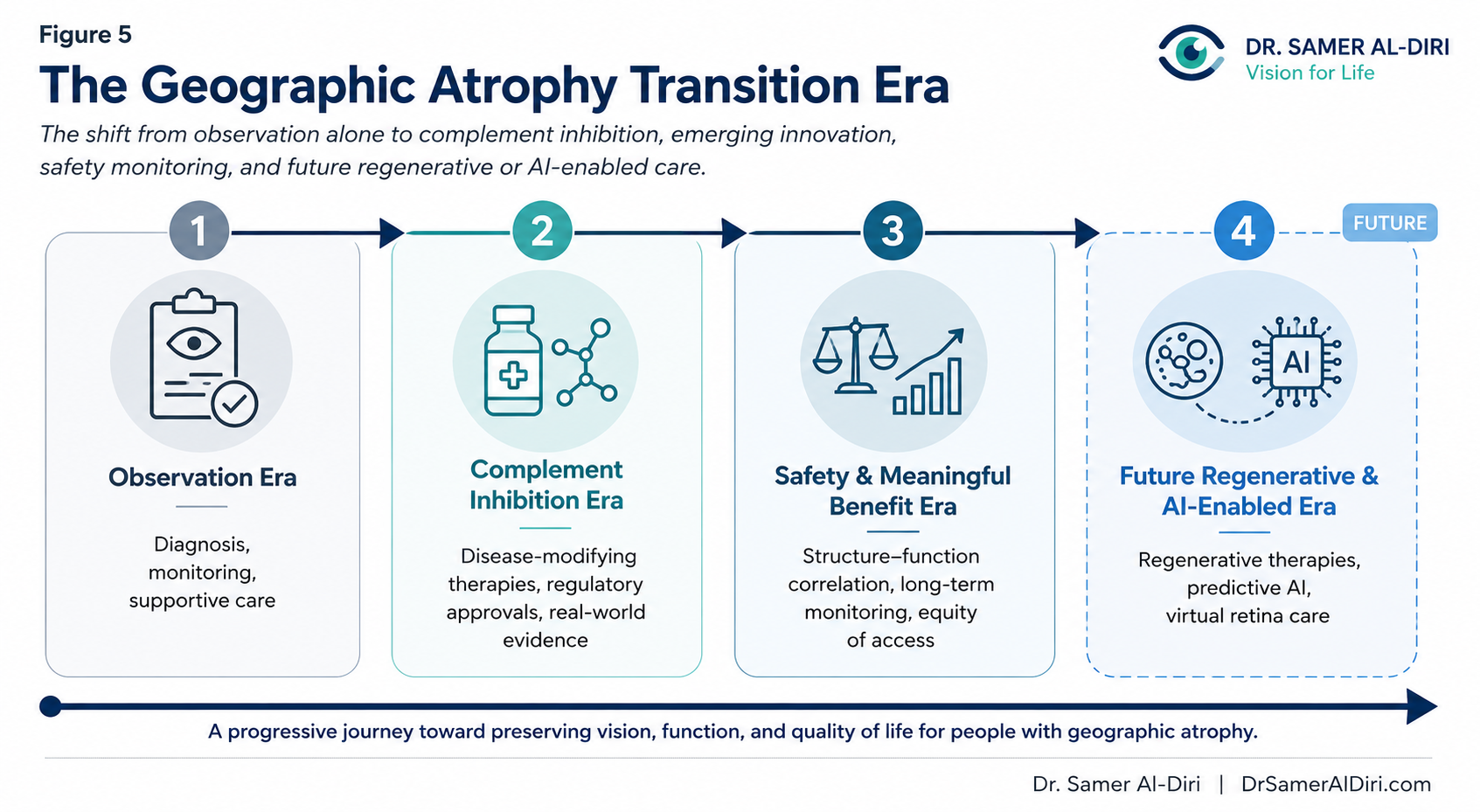
Figure 5. The Geographic Atrophy Transition Era: ageing populations, improved detection, emerging GA therapies, monitoring requirements, and service-capacity pressures are reshaping the future of AMD care.
The Economic Burden of AMD
The burden of AMD extends far beyond direct healthcare expenditure. The disease generates substantial costs through clinic visits, imaging, treatments, rehabilitation services, visual disability, social care requirements, and informal caregiving. A recent multinational cost-of-illness study estimated a substantial annual economic burden for late-stage AMD, including tens of billions of dollars in the United States when direct medical, indirect medical, productivity, and wellbeing costs were included [16]. However, direct medical costs represent only part of the overall burden. Indirect costs associated with reduced productivity, caregiver support, transportation requirements, loss of independence, falls, disability, and institutional care contribute substantially to the wider economic impact. More broadly, global productivity losses attributable to vision impairment and blindness have been estimated to exceed US$400 billion annually [7]. Investment in sustainable vision care should be considered not only a healthcare expenditure but also a long-term societal investment.
Equity, Access, and Workforce Reality
Scientific advances cannot improve outcomes if patients cannot access care. Workforce distribution remains highly unequal across regions. International data suggest that ophthalmologist density may exceed 10–20 per 100,000 population in some high-income countries while remaining below 1 per 100,000 population in parts of sub-Saharan Africa and other resource-constrained settings [17]. Retina subspecialty capacity is often even more limited. For many patients, access to AMD diagnosis and treatment depends as much on workforce availability as on scientific innovation. These disparities are a health-equity challenge, not simply a service-planning problem.
Workforce Mathematics and the Vision-Care Capacity Gap
The challenges facing AMD care are captured by two concepts discussed earlier in this work: Workforce Mathematics and the Vision-Care Capacity Gap. Workforce Mathematics recognises a fundamental reality: if patient demand grows faster than workforce capacity, access pressures become inevitable regardless of scientific progress. The Vision-Care Capacity Gap describes the widening mismatch between the number of individuals requiring care and the resources available to deliver that care. AMD represents a particularly powerful example of this phenomenon. Unless addressed proactively, this mismatch risks becoming one of the defining healthcare challenges of ageing societies.
The Implementation Chasm
The existence of effective interventions does not guarantee effective delivery. The challenge is reflected in the Implementation Chasm discussed later in this work. For AMD, delays in diagnosis, treatment initiation, follow-up monitoring, or access to emerging therapies may directly influence visual outcomes. The challenge facing health systems is not merely discovering new treatments but ensuring that scientific advances reach patients in a timely and equitable manner.
Patient Perspective: When Capacity Becomes Personal
Consider Mr. P, a 76-year-old retired engineer with bilateral Geographic Atrophy. After noticing increasing difficulty reading and recognising faces, he was referred for specialist assessment. Because of workforce shortages and clinic backlogs, his first retinal appointment was scheduled several months later. During this period, his visual function continued to deteriorate. For health-system planners, waiting times may appear as operational metrics. For patients, they represent time during which visual function, independence, and quality of life may be irreversibly lost. Unlike many other tissues, retinal tissue lost to advanced AMD cannot currently be restored. From the patient perspective, delays are not administrative inconveniences; they may influence lifelong visual outcomes.
Health-System Resilience and AMD
The growing burden of AMD raises a broader question: how resilient are health systems to the pressures created by population ageing? Health-system resilience refers to the ability of healthcare systems to absorb rising demand, adapt to emerging challenges, and maintain high-quality care over time. AMD provides an important test of that resilience. Health systems that fail to anticipate these pressures may face widening waiting lists, increasing inequalities, workforce burnout, and reduced quality of care.
Implications for Future AMD Care
Meeting the future challenge of AMD will require a shift from reactive care towards strategic system planning. Many of these challenges are addressed within The Sustainable Vision Care Framework. It provides a strategic model for translating scientific innovation into sustainable population-level benefit. However, implementation will require coordinated action across multiple sectors. The future challenge of AMD is therefore not solely scientific – it is organisational, economic, demographic, and political.
Key Message
The health-system impact of AMD extends far beyond ophthalmology clinics. It influences workforce requirements, imaging infrastructure, outpatient capacity, healthcare expenditure, rehabilitation services, and long-term sustainability. As populations age and new therapies emerge, the central question is no longer whether AMD can be treated, but whether health systems can deliver timely, equitable, and sustainable care at the scale required. Geographic Atrophy makes that question more urgent.
Geographic Atrophy: The New Therapeutic Era and the Challenge of Meaningful Benefit
Geographic Atrophy (GA) represents the advanced atrophic form of age-related macular degeneration (AMD) and a major cause of irreversible central vision loss among older adults worldwide. Characterised by progressive degeneration of the retinal pigment epithelium (RPE), overlying photoreceptors, and underlying choriocapillaris, GA leads to sharply demarcated areas of retinal tissue loss that enlarge over time and ultimately compromise reading, face recognition, mobility, and independence [66].
Those of us who have treated AMD for years remember the old GA conversation. We could explain the diagnosis. We could show the atrophy on imaging. We could offer monitoring, low-vision rehabilitation, and risk-factor advice. But we could not offer a treatment that altered the course of disease. That therapeutic void bred a form of clinical nihilism: explanation without intervention.
That era has ended.
Complement-inhibitor therapies have moved GA from observation alone toward active disease modification. That is a real shift. Yet it is not a simple triumph. The benefit is modest, the functional impact remains contested, the treatment burden is substantial, and safety, access, and workforce implications are impossible to ignore.
The Complement Pathway as a Therapeutic Target
Genetic, histologic, and biomarker studies have implicated chronic dysregulation of the complement alternative pathway in the pathogenesis of GA. Overactivation of the complement cascade leads to inflammation, cell lysis, and progressive retinal tissue loss. Two key nodes in the cascade – complement component 3 (C3) and complement component 5 (C5) – have been successfully targeted by intravitreal therapies.
Pegcetacoplan (Syfovre)
Pegcetacoplan is a synthetic cyclic peptide that binds to C3 and its activated fragment C3b, inhibiting all downstream complement activation pathways. It received United States Food and Drug Administration (FDA) approval in February 2023 for the treatment of GA secondary to AMD – the first approved therapy for this indication [19].
Pivotal trials: OAKS and DERBY
The phase 3 OAKS and DERBY trials enrolled over 1,500 patients with GA secondary to AMD. Participants received monthly or every-other-month intravitreal pegcetacoplan or sham injections for 24 months. Both trials met their primary endpoint: statistically significant slowing of GA lesion growth compared with sham [25].
At 24 months, lesion growth rate reductions were approximately 20-25% for monthly dosing and 17-21% for every-other-month dosing, with effects becoming more apparent over time. Yet no statistically significant improvement in best-corrected visual acuity, low-luminance visual acuity, or patient-reported functional outcomes was demonstrated during the primary analysis period.
Safety signals
The most common adverse events were typical of intravitreal injections, including conjunctival haemorrhage and increased intraocular pressure. However, a notable safety signal emerged for pegcetacoplan: intraocular inflammation (IOI) and rare post-marketing reports of retinal vasculitis and/or retinal vascular occlusion, sometimes associated with severe vision loss. The current FDA label includes a warning for retinal vasculitis and/or retinal vascular occlusion. Clinicians should monitor carefully for inflammation after treatment and discontinue therapy if these events occur [19,25].
Avacincaptad Pegol (Izervay)
Avacincaptad pegol is a complement C5 inhibitor that blocks the cleavage of C5 to C5a and C5b, thereby inhibiting the terminal complement pathway. It received FDA approval in August 2023 for GA secondary to AMD [28].
Pivotal trial: GATHER2
The phase 3 GATHER2 trial enrolled approximately 450 patients, randomising them to monthly avacincaptad pegol or sham for 12 months. The study met its primary endpoint, showing a statistically significant reduction in GA lesion growth (approximately 20-30%) at 12 months [26]. Supportive data from the earlier phase 2/3 GATHER1 trial (18-month results) showed similar slowing [27].
Safety signals
In GATHER2 and current FDA labelling, avacincaptad pegol should not be presented as having a retinal vasculitis risk comparable to pegcetacoplan. Its key safety considerations include standard intravitreal injection risks, contraindication in ocular/periocular infection or active intraocular inflammation, and warnings relating to endophthalmitis, retinal detachment, neovascular AMD, and increased intraocular pressure. Careful patient counselling, post-injection monitoring, and ongoing pharmacovigilance remain essential [26,28].
The Structure–Function Challenge
The most difficult unresolved question in GA therapeutics is the gap between anatomical slowing and functional benefit. The Structure–Function Challenge captures this uncertainty: does reducing the rate of lesion enlargement preserve the things patients actually fear losing — reading, face recognition, mobility, independence? Opinion differs sharply. Some clinicians argue that slowing atrophy is meaningful because lost retinal tissue cannot be replaced. Others worry that without demonstrable preservation of reading or daily function, we risk treating scans rather than lives. Both concerns deserve serious attention.
In the OAKS and DERBY trials, pegcetacoplan slowed lesion growth by 20-25% but did not demonstrate statistically significant improvements in best-corrected visual acuity, low-luminance visual acuity, reading speed, or patient-reported outcomes at 24 months [25]. Similar observations apply to avacincaptad pegol [26]. Post-hoc analyses suggest possible functional signals in subgroups (e.g., non-subfoveal GA or fast progressors), but these are not definitive.
The Structure–Function Challenge has profound regulatory and clinical consequences. The FDA approved complement inhibitors based on structural endpoints; the EMA refused marketing authorisation for pegcetacoplan citing insufficient functional evidence [20]; NICE discontinued its appraisal [21]. For patients and clinicians, the challenge is shared decision-making: a slower-growing lesion that does not demonstrably preserve visual function may still be valued by some, but not by others.
Addressing the Structure–Function Challenge will require future trials to incorporate validated functional endpoints, patient-reported outcome measures, and longer follow-up. It also highlights the need for better biomarkers that predict which patients are most likely to derive functional benefit.
Safety and Responsible Innovation
The safety profiles of complement inhibitors require transparent discussion. Pegcetacoplan has been associated with intraocular inflammation and rare but serious post-marketing cases of retinal vasculitis and/or retinal vascular occlusion, now reflected in FDA labelling [19]. Avacincaptad pegol shares the general risks of intravitreal injection and requires careful monitoring, but current FDA labelling does not include a comparable retinal vasculitis warning [28].
Safety is not an abstract regulatory paragraph for patients. It is the question they carry into the consent conversation: “What might this do to my eye, and what happens if something goes wrong?” Anxiety before the next injection can be real. Honest counselling matters as much as technical skill.
Responsible innovation demands:
– Pre-treatment counselling about potential benefits, burdens, and risks.
– Vigilant monitoring for signs of inflammation after each injection.
– Prompt investigation and management of any suspected IOI.
– Reporting of adverse events to registries and regulators.
These safety considerations do not negate the value of complement inhibitors, but they reinforce the need for careful patient selection, shared decision-making, and ongoing real-world data collection.
Regulatory Divergence and Real-World Access
Regulatory interpretation of Geographic Atrophy (GA) therapies now differs across major jurisdictions. The table below is a snapshot, not a guarantee. Approval, reimbursement, procurement, safety monitoring, and on-the-ground access vary widely; local regulatory and commissioning status should always be verified before clinical or policy decisions are made.
Table – Global regulatory-access snapshot for Geographic Atrophy therapies
| Jurisdiction / region | Agency and current status | Access and policy interpretation |
| United States | FDA – pegcetacoplan and avacincaptad pegol are approved for GA secondary to AMD [19,28]. | The FDA accepted structural GA lesion-growth endpoints, but real-world use still depends on payer policy, safety monitoring, clinic capacity, and shared decision-making. |
| European Union | EMA – Syfovre (pegcetacoplan) received a refusal of marketing authorisation; Izelvay (avacincaptad pegol) application was withdrawn after unresolved concerns [20,67]. | The EMA decision reflects a higher threshold for clinically meaningful benefit when functional outcomes remain uncertain. |
| England | NICE – pegcetacoplan appraisal ID4041/GID-TA11351 was discontinued rather than issued as completed final technology appraisal guidance [21]. | NICE illustrates the distinction between scientific authorisation, health-technology assessment, affordability, and practical NHS adoption. |
| Australia | TGA – Syfovre was registered in January 2025 and Izervay was registered in October 2025 for defined adult GA populations [68,69]. | Australian registration widens the global access map, although reimbursement, procurement, and service capacity will determine actual patient reach. |
| Japan | MHLW / PMDA pathway – Astellas reported conditional approval of Izervay in September 2025 for suppression of GA growth in atrophic AMD [70]. | Japan’s pathway shows that conditional or staged access can be used when unmet need is high but longer-term evidence continues to mature. |
| China | NMPA / CDE – Astellas reported that the Izervay NDA was accepted and granted Priority Review in May 2026; approval was not presented as final in this review [71]. | Priority review in China signals regulatory momentum, but national approval, pricing, hospital adoption, and regional equity will shape real access. |
| South Korea | MFDS – no product-specific public approval for GA complement inhibitors was identified in this review; local status should be verified at the time of use [72]. | No public confirmation should not be read as absence of future access; reimbursement and local evidence review will determine adoption. |
| Africa | AMA / national regulators – AMA became operational in 2025; WHO–AMA collaboration launched in 2026 to support regulatory harmonisation [73,74]. | Access will depend on national regulators, procurement, specialist capacity, and affordability rather than a single continental decision. |
| South America | PAHO / national authorities – regulatory decisions remain country-specific, including through ANMAT, ANVISA, INVIMA, ISP and others [75]. | Regional access will depend on national approval, pricing, reimbursement, retina-service capacity, and procurement. |
Access therefore differs substantially across jurisdictions. The global picture reinforces a central argument of this work: scientific efficacy is only one component of patient benefit. Meaningful access also depends on regulatory interpretation, reimbursement decisions, clinical infrastructure, workforce capacity, patient selection, and the ability of health systems to monitor real-world outcomes safely and equitably.
The Emerging Therapeutic Pipeline
Complement inhibition is only the first chapter. The GA pipeline now includes:
– Gene therapy – JNJ-81201887 (AAVCAGsCD59, phase 2), OCU410 (phase 1/2), and GT005 (EXPLORE) illustrate efforts to provide durable complement modulation with a single intravitreal or subretinal administration. The discontinuation of GT005 (Novartis, 2023) reminds us that not all gene therapy programmes succeed [47–49,51].
– Cell replacement – OpRegen (RG6501, phase 1/2a) is an allogeneic RPE cell suspension delivered subretinally. Early reports show long-term structural and functional stability in some treated patients, but larger controlled trials are needed [50].
– Retinal prosthesis – The PRIMA photovoltaic implant (phase 2, NEJM 2026) has restored partial central reading vision in patients with end-stage GA, representing a restorative paradigm rather than a disease-slowing one [29].
– Neuroprotection and combination approaches – Multiple mechanisms (e.g., mitochondrial protectants, anti-inflammatory agents) are in early development.
The future of GA care will likely involve precision selection – matching patients to the right therapy based on genetics, imaging biomarkers, and progression rate – rather than a one-size-fits-all approach.
Beyond complement inhibition, gene therapy, cell replacement, and retinal implants, several additional approaches are now in clinical testing. Elamipretide, a mitochondrial-targeted peptide, did not meet its primary ReCLAIM-2 endpoints but reported exploratory signals of reduced progression of ellipsoid-zone attenuation [54]; it is being evaluated in the phase 3 ReNEW study (NCT06373731) for dry AMD/GA [55]. Tinlarebant, an oral RBP4 inhibitor designed to reduce toxic lipofuscin accumulation, is being evaluated in the phase 3 PHOENIX study (NCT05949593) for GA [56]. Vonaprument (ANX007), a C1q inhibitor targeting the classical complement pathway, is being evaluated in a phase 3 study (NCT06510816) [57], while cemdisiran, an RNAi therapeutic targeting C5, is being studied alone or in combination with pozelimab in a phase 3 GA trial (NCT06541704) [58]. These diverse mechanisms – from mitochondrial protection and visual-cycle modulation to alternative complement targeting – highlight the rapidly expanding therapeutic landscape for GA beyond first-generation complement inhibitors.
Evidence-Based Hope in AMD
A Realistic Path Forward
For decades, AMD – and especially Geographic Atrophy – was described as untreatable. That narrative is no longer accurate, but neither is unrealistic optimism. Evidence-based hope occupies the middle ground: acknowledging genuine scientific progress while being transparent about current limitations.
Why Hope Matters
Hope is not a substitute for evidence; it is a prerequisite for patient engagement, research investment, and health-system planning. Patients who understand what is possible – and what is not – are more likely to adhere to monitoring, accept reasonable treatment burdens, and participate in clinical trials.
What Is Established
– Complement inhibitors (pegcetacoplan, avacincaptad pegol) slow GA lesion growth by approximately 20-30% across pivotal one- to two-year trial timeframes, with systematic-review evidence supporting anatomical benefit but not yet consistent functional improvement [25,26,52]. This is real, measurable progress.
– Artificial intelligence can predict conversion to neovascular AMD with high accuracy and is beginning to forecast GA progression rates and quantify GA from OCT imaging [23,24,30].
– Retinal implants (PRIMA) have restored partial central reading vision in selected patients with end-stage GA, with patient-facing summaries now helping communicate this emerging field to affected communities [29,43].
– Home OCT and teleophthalmology are making routine monitoring more accessible and less burdensome [31].
– Low-vision rehabilitation can substantially improve functional independence and quality of life for people with advanced vision loss [12].
What Is Emerging but Not Yet Routine
– Gene therapy (JNJ-81201887, OCU410) aims to provide durable complement modulation with a single administration. Early phase results are promising, but larger, longer trials are needed [47,48].
– Cell replacement (OpRegen/RG6501) – allogeneic RPE transplantation – has shown structural and functional stability in some patients [50].
– Combination therapies (complement inhibitor plus neuroprotection or anti-inflammatory agents) are in early development.
– Precision medicine – selecting patients based on genetics, imaging biomarkers, or progression rate – may improve the risk-benefit ratio of existing and future therapies.
What Remains Uncertain
– Does slowing GA growth preserve functional vision (reading, mobility, independence)? (The Structure–Function Challenge)
– What is the optimal duration of complement inhibitor therapy?
– Which patient subgroups derive the greatest benefit?
– Will one-time gene or cell therapies prove safe and durable?
– How can workforce and capacity gaps be closed before GA treatment demand overwhelms services?
Unanswered Questions
What I still do not know — and what the field urgently needs to answer — is whether earlier GA treatment changes lived experience over five or ten years, not just lesion growth over one or two. Do patients read for longer? Drive safely for longer? Stay independent for longer? We need longer follow-up, better patient-reported outcomes, real-world registries, and a more honest reckoning with treatment burden.
There are also system-level questions. Which patients should be prioritised when capacity is limited? How should payers value anatomical slowing without clear functional gain? How do we protect equity when new therapies require repeated visits, imaging, and specialist oversight? These questions do not weaken the case for innovation. They make the case for better evidence and better planning.
What Hope Does Not Promise
– Cure.
– Restoration of lost vision (except for highly selected implant recipients).
– Elimination of treatment burden.
– Immediate universal access.
The Core Message
Patients and clinicians should neither accept therapeutic nihilism nor expect a miracle. They should engage with the evidence, advocate for functional outcomes in future trials, support post-marketing registries, and plan health systems to deliver the best of today’s care while preparing for tomorrow’s advances.
Evidence-based hope is not a compromise; it is the only responsible way forward.
Workforce Pressures, Capacity Constraints, and the Vision-Care Capacity Gap
Why Workforce Capacity Matters
Scientific advances have transformed the diagnosis and management of age-related macular degeneration (AMD). New imaging technologies, anti-vascular endothelial growth factor (anti-VEGF) therapies, artificial intelligence (AI) applications, and emerging treatments for Geographic Atrophy (GA) have created unprecedented opportunities to preserve vision and improve patient outcomes. However, scientific progress alone cannot guarantee population-level benefit.
Every diagnostic test, clinic visit, retinal image, treatment injection, and follow-up appointment ultimately depends upon a healthcare workforce capable of delivering care. The future impact of AMD will therefore depend not only on therapeutic innovation, but also on whether health systems have the workforce capacity to implement that innovation at scale.
The challenge facing many healthcare systems is increasingly clear: patient demand is rising faster than workforce capacity. As discussed in the previous chapter on Health-System Impact, ophthalmology has become one of the busiest outpatient specialties in many countries, with more than eight million ophthalmology outpatient appointments annually reported within NHS England alone [14]. Against this backdrop, AMD represents one of the most workforce-intensive chronic conditions in modern ophthalmology.
Workforce Mathematics
One of the central analytical lenses used in this work is Workforce Mathematics. Workforce Mathematics describes the relationship between patient demand, service capacity, workforce availability, clinical workload, and health-system performance. At its simplest:
Patient Demand > Workforce Capacity = Vision-Care Capacity Gap

Figure 6. A New Standard of Care: integrated AMD care requires coordinated early detection, ongoing monitoring, treatment decisions, rehabilitation, workforce capacity, digital innovation, and patient-centred outcomes.
The equation appears deceptively simple. Yet it captures one of the central realities facing future AMD care. If the number of patients eligible for Geographic Atrophy treatment rises by 20% over five years while workforce capacity expands by only 2-3% annually, a service imbalance becomes increasingly likely.
This illustrates a fundamental principle of Workforce Mathematics: Scientific innovation can increase demand faster than health systems can expand delivery capacity.
Unlike pharmaceutical development, workforce expansion cannot be accelerated rapidly. Training pathways require years, infrastructure requires investment, and specialist expertise takes time to develop. Workforce planning must therefore become a core component of future AMD strategy rather than a secondary operational consideration.
Workforce Mathematics in Practice – Consider a hypothetical health system employing 200 retina specialists. If AMD-related demand increases by 40% by 2035 while workforce growth reaches only 10%, the system may require approximately 280 retina specialists but have only 220 available. The result is a shortfall of approximately 60 specialists despite ongoing recruitment efforts. This simple example demonstrates how modest annual imbalances can generate substantial long-term capacity deficits.
The Vision-Care Capacity Gap
The capacity gap described earlier is increasingly visible across many healthcare systems. Population ageing is increasing the number of people living with AMD, while therapeutic advances are increasing the intensity of care required for many patients. Imaging volumes continue to rise. Treatment pathways become more complex. Expectations about access and outcomes keep growing. The result is a widening divergence between demand and delivery capacity. This is not merely an operational problem; it is a threat to equity, access, quality of care, and long-term health-system sustainability.
Patient Perspective – For a patient with rapidly progressing Geographic Atrophy, a six-month delay in specialist assessment or treatment due to workforce shortages may result in irreversible retinal tissue loss. Unlike many chronic conditions, retinal tissue lost to advanced AMD cannot currently be restored. From the patient perspective, workforce shortages are not abstract health-system problems. They may directly influence lifelong visual outcomes.
Geographic Atrophy as a Capacity Multiplier
Disease-modifying therapies for Geographic Atrophy have begun to change a field long defined by observation, monitoring, and supportive care. They also create a different service model. Regular intravitreal treatment, repeated imaging, safety monitoring, patient counselling, and long-term follow-up all require workforce capacity. Even if only a minority of eligible GA patients receive treatment, the cumulative effect on retinal services could be considerable. GA therefore functions not only as a clinical challenge, but also as a workforce and capacity multiplier. Biological efficacy will matter. So will implementation capacity.
The Global Workforce Reality
The workforce challenge is not confined to any single country. International workforce data demonstrate substantial variation in ophthalmologist density across regions. In some high-income countries, ophthalmologist density exceeds 10-20 specialists per 100,000 population. In contrast, many low-income countries report fewer than one ophthalmologist per 100,000 population [17,18]. Retina subspecialists are considerably rarer. In many regions, a single retina specialist may serve hundreds of thousands – or even millions – of people. These disparities highlight the uneven global capacity available to manage future AMD demand. Scientific innovation cannot deliver equitable outcomes if specialist services remain inaccessible to large segments of the global population.
The Training Pipeline Challenge
Expanding workforce capacity is not a rapid process. Even when governments or healthcare organisations recognise shortages, solutions may take many years to materialise. A future retina specialist must complete medical training, ophthalmology residency or specialty training, subspecialty fellowship training, and supervised clinical practice before becoming fully independent. In many healthcare systems, this may require five to seven years or longer after entry into ophthalmology training. The mismatch is structural: service demand can rise quickly, but workforce expansion moves slowly. The workforce decisions made today will largely determine capacity available a decade from now.
The Retirement Wave
A further challenge receives comparatively little attention: the ageing of the ophthalmology workforce itself. Many experienced retina specialists currently providing AMD care are approaching retirement age. Healthcare systems face a dual challenge: rising patient demand and potential loss of experienced clinicians. Workforce planning must address not only future demand growth but also replacement of existing expertise. If this retirement wave is ignored, shortages may appear even in systems that currently seem adequately staffed.
The Capacity Paradox
The future of AMD care is increasingly shaped by a capacity paradox. Scientific progress improves diagnostics, identifies more patients earlier, expands treatment eligibility, and increases opportunities for intervention. Yet those successes also generate service demand. Better diagnostics identify more patients. Improved treatments create more individuals requiring ongoing monitoring. New therapeutic pathways increase clinic activity. Patient expectations rise as treatment options expand. Scientific progress may therefore increase demand faster than healthcare systems can expand delivery capacity.
Can Technology Solve the Workforce Problem?
Technology will play a central role in future capacity expansion. AI can assist with image interpretation, triage, risk stratification, workflow optimisation, and clinical decision support. Digital platforms may improve monitoring efficiency and make virtual care more practical. But technology alone will not solve workforce shortages. Every AI system still needs governance, oversight, validation, maintenance, and clinical integration. A useful multiplier, yes. A replacement for trained clinical judgement, no.
Task-Shifting and Service Redesign
Technology represents only one component of future capacity expansion. Other proven approaches include: nurse-led injection clinics, optometrist-led monitoring programmes, allied-health professional support models, virtual review clinics, and AI-assisted image triage pathways. When supported by appropriate governance, training, quality assurance, and regulatory oversight, these strategies may substantially increase service capacity while maintaining patient safety. Workforce redesign may often be achieved more rapidly than workforce expansion. As a result, service redesign is likely to become an increasingly central component of sustainable AMD care.
Workforce Pressures and the Implementation Chasm
Effective therapies do not guarantee access. That is the Implementation Chasm in practice. Workforce shortages, funding constraints, infrastructure limitations, and operational bottlenecks can slow adoption even when the science is sound. GA illustrates the problem clearly. Without workforce development and service redesign, even a clinically useful therapy may fail to reach the people who need it.
Patient Vignette: When Workforce Shortages Become Personal
Consider Mr. R, a 72-year-old retired accountant living with bilateral Geographic Atrophy. After referral for specialist assessment, workforce shortages and clinic backlogs resulted in a prolonged wait before his retinal consultation. During this period, reading became increasingly difficult, driving was abandoned, and confidence in daily activities declined. For healthcare administrators, workforce shortages may appear as vacancy rates, staffing gaps, or performance metrics. For patients such as Mr. R, workforce shortages are experienced differently. They are measured in delayed diagnoses, postponed treatment decisions, lost independence, and irreversible vision loss. This distinction highlights why workforce planning must remain fundamentally patient-centred.
A Strategic Planning Perspective
The future challenge of AMD is increasingly predictable. Population ageing trends, workforce demographics, therapeutic developments, and rising service demand are already visible. This creates a unique opportunity for proactive planning. Health systems that invest early in workforce development, service redesign, digital infrastructure, implementation capacity, and innovative care models are likely to be better positioned to respond to future AMD demand. Those that delay adaptation may experience widening Vision-Care Capacity Gaps despite continuing scientific progress.
Implications for Future AMD Care
Many of these challenges are addressed within The Sustainable Vision Care Framework, particularly through its pillars of workforce development, technological innovation, equitable access, rehabilitation, health-system resilience, and implementation capacity. The framework recognises a critical reality: scientific breakthroughs achieve population-level impact only when supported by sufficient workforce and delivery infrastructure. The future of AMD care will therefore depend as much on workforce planning and health-system design as on therapeutic discovery.
Key Message
The future challenge of AMD is not solely scientific. It is fundamentally a workforce challenge. Population ageing, Geographic Atrophy therapies, increasing imaging demands, and growing treatment complexity are creating pressures that many healthcare systems are not yet prepared to absorb. Health-system leaders must commission workforce forecasts, expand training pathways, support task-shifting, invest in AI-enabled capacity multipliers, and strengthen implementation infrastructure now. Every year of delay widens the Vision-Care Capacity Gap, increases pressure on services, and risks preventable vision loss for future generations of patients.
The Implementation Chasm
Why Scientific Innovation Often Fails to Reach Patients at Scale
Introduction
Modern medicine has entered an era of extraordinary scientific innovation. Advances in retinal imaging, artificial intelligence, precision diagnostics, intravitreal therapies, gene therapy, and digital health technologies are transforming the possibilities of vision care. Yet an important paradox exists. Scientific progress does not automatically translate into population benefit – a truth often overlooked in the excitement surrounding breakthrough clinical trials.
Many innovations work in studies and still fail to reach the people who need them. I think of that gap as the Implementation Chasm.
The Implementation Chasm is the distance between scientific possibility and real-world patient benefit. It is not a failure of discovery. It is a failure of systems — workforce, infrastructure, financing, regulation, procurement, digital integration, and equitable access.
As medical innovation accelerates, the ability of healthcare systems to close this gap may become as central as innovation itself. Implementation-science research has long recognised that delays often occur between scientific discovery and routine clinical adoption. Across healthcare disciplines, evidence suggests that more than a decade may separate breakthrough research from widespread implementation. For AMD, the Implementation Chasm is therefore not only a gap in access. It is a gap in time.
One practical way to narrow the implementation gap is to move appropriate elements of monitoring, education, triage, and support closer to patients while preserving specialist oversight.
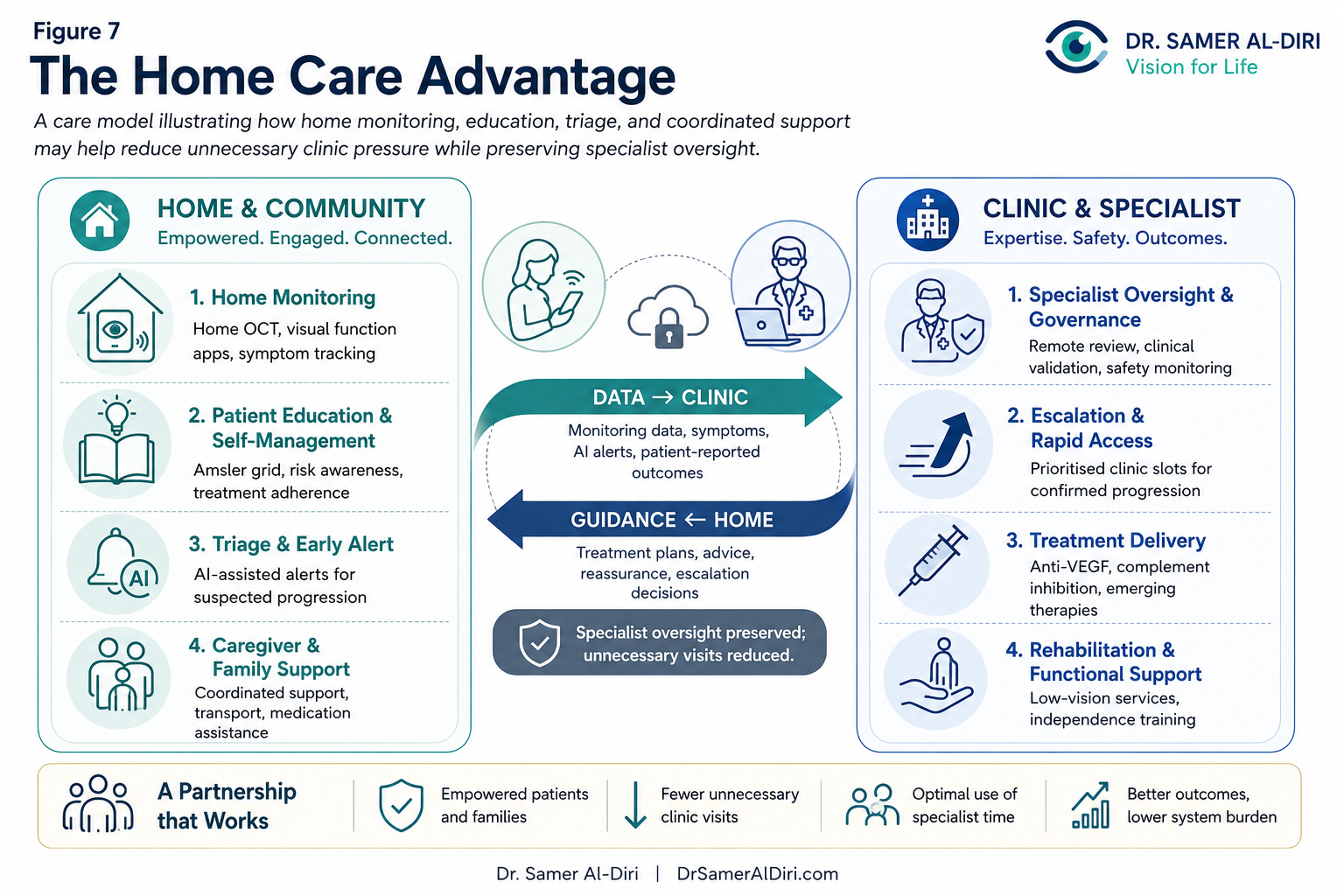
Figure 7. The Home Care Advantage: home-based monitoring, virtual care, patient education, and timely escalation can support earlier detection, reduce unnecessary clinic visits, improve continuity of care, and keep AMD care closer to patients.
The Innovation-Implementation Paradox
Medical innovation is often viewed as a linear process: Research → Evidence → Approval → Adoption → Patient Benefit. In reality, the pathway is rarely so straightforward. Many effective innovations encounter barriers including workforce shortages, infrastructure limitations, funding constraints, regulatory divergence, reimbursement delays, geographic inequities, organisational inertia, and digital integration challenges. As a result, scientific success does not guarantee population-level impact. This creates the Innovation-Implementation Paradox: an intervention may be clinically effective while simultaneously remaining inaccessible to large numbers of patients.
Geographic Atrophy as a Contemporary Example
Geographic Atrophy provides one of the clearest examples of the Implementation Chasm in contemporary retinal care. For decades, GA represented one of the largest unmet needs in ophthalmology. The emergence of complement-inhibitor therapies therefore marked a major scientific milestone. However, approval alone does not guarantee implementation. Successful delivery requires early identification of eligible patients, imaging capacity, specialist assessment, treatment infrastructure, workforce availability, long-term monitoring, and sustainable funding pathways. Each component may create potential barriers.
The evolution of GA treatment provides a real-time illustration. Pegcetacoplan (Syfovre) received FDA approval in 2023 as the first approved therapy for GA [19]. Implementation pathways then diverged. Patients in the United States gained access to treatment, while the European Medicines Agency declined marketing authorisation and NICE later discontinued its appraisal process [20,21]. A patient who might have been eligible in one jurisdiction had no equivalent access in another. The science was identical. The implementation outcome was not.
Regulatory Approval Is Only the Beginning
The journey from scientific discovery to patient benefit involves multiple stages: Scientific Evidence → Regulatory Evaluation → Reimbursement and Funding → Service Implementation → Workforce Readiness → Patient Access. Failure at any stage may widen the Implementation Chasm. The impact of implementation can be illustrated through a simple example: imagine a therapy capable of reducing disease progression by 25%. If only 30% of eligible patients receive treatment, the population-level benefit falls substantially below its scientific potential. Conversely, increasing coverage from 30% to 70% could more than double real-world impact without requiring any additional scientific breakthrough. Closing the Implementation Chasm may therefore generate population-level benefits comparable in importance to some therapeutic advances.
Visualising the Implementation Chasm
The Implementation Chasm may be conceptualised as a series of filters: Discovery → Evidence Generation → Regulatory Approval → Reimbursement and Funding → Workforce Capacity → Infrastructure Readiness → Patient Access → Equitable Population Benefit. At each stage, potential beneficiaries may be lost. The largest barriers are often organisational rather than scientific.
The Implementation Chasm by the Numbers
Across medicine, it can take a decade or more for proven interventions to become routine care. Even after approval, reimbursement delays, staffing shortages, infrastructure gaps, and referral failures mean that many eligible patients never receive optimal treatment. Closing those delivery gaps can improve population outcomes as much as a modest increase in drug efficacy — an uncomfortable truth for a field that often celebrates discovery more than delivery.
AMD Is Not Unique
The Implementation Chasm is not unique to AMD. Similar delays have been documented in cancer immunotherapy, cardiovascular innovation, gene therapy, and precision medicine. However, AMD presents a particularly compelling example because disease progression is frequently irreversible, treatment opportunities may be time-sensitive, and delayed access can directly influence long-term visual function, independence, and quality of life.
Regulatory Divergence and Real-World Consequences
The GA treatment landscape illustrates how implementation barriers may emerge even after scientific progress. Different regulatory agencies interpret evidence differently. The contrasting approaches of the FDA and EMA regarding complement-inhibitor therapies highlight how differing interpretations of structural and functional outcomes can influence patient access. This is not merely a theoretical divergence – it has influenced access to treatment for patients across different healthcare systems and demonstrates how governance and policy decisions can shape clinical reality.
Workforce Limitations as an Implementation Barrier
Workforce constraints represent one of the most important contributors to the Implementation Chasm. A therapy may be effective, approved, and funded, yet still fail to reach patients if healthcare systems lack retina specialists, nurses, imaging personnel, clinic capacity, or administrative support. The challenge directly connects to Workforce Mathematics and the Vision-Care Capacity Gap. The Implementation Chasm therefore represents one practical consequence of the Vision-Care Capacity Gap. Workforce development should be viewed as an integral component of innovation strategy rather than a separate operational issue.
Infrastructure Matters
Modern AMD care depends upon infrastructure: imaging equipment, digital systems, data storage, clinical space, and treatment facilities. Healthcare systems with limited infrastructure may struggle to implement innovations efficiently regardless of scientific merit. Conversely, systems with strong infrastructure may adopt innovations more rapidly and effectively. Infrastructure functions as a major determinant of implementation success.
The Equity Dimension
The Implementation Chasm does not affect all populations equally. Groups at greater risk of exclusion include rural populations, underserved communities, low-income groups, ethnic minorities, individuals with limited mobility, and residents of low- and middle-income countries. Innovation without equity risks widening disparities. Equity without innovation risks stagnation. The future of AMD care requires both.
Patient Perspective – Mr. T is a 72-year-old patient with bilateral Geographic Atrophy. After learning about a newly approved therapy, he attends a specialist consultation and is deemed clinically eligible. However, reimbursement delays, travel requirements, and administrative barriers prolong access for several months. During this period, disease progression continues. The therapy exists. The evidence exists. The patient remains untreated. This is the human face of the Implementation Chasm.
The Economic Cost of the Chasm
The cost of the Implementation Chasm is not measured solely in delayed access. It is also measured in avoidable disease progression. Each month of delayed diagnosis, delayed treatment, or delayed implementation may allow additional irreversible retinal damage to occur. These delays may increase future rehabilitation needs, caregiver burden, healthcare utilisation, and social-care costs. The economic cost includes both unrealised benefit and avoidable harm.
Artificial Intelligence and the Implementation Chasm
Artificial intelligence has the potential to reduce certain implementation barriers through automated image interpretation, risk stratification, referral optimisation, workflow management, and remote monitoring. It does not remove the challenge. AI itself requires governance, validation, workforce training, digital infrastructure, and clinical integration. It may narrow or widen implementation gaps depending on how it is deployed. The safest view is to treat AI as a tool for reducing the Implementation Chasm, not as a way to make it disappear.
Closing the Implementation Chasm
Reducing the Implementation Chasm requires coordinated action across multiple domains: proactive workforce development and strategic capacity planning, harmonised regulatory and reimbursement pathways, expanded imaging and treatment infrastructure, teleophthalmology and community-based delivery models, patient-navigation programmes that reduce non-medical barriers, real-world evidence registries that accelerate implementation, and AI-enabled service redesign supported by well-designed governance. The objective is not merely to accelerate innovation – it is to accelerate access.
Who Is Responsible for Closing the Chasm? – Responsibility is distributed across multiple stakeholders: regulators and health-technology assessment bodies influence approval and reimbursement decisions; governments and health ministries influence workforce development, financing, and infrastructure investment; healthcare organisations influence service design and operational efficiency; clinical leaders influence adoption, quality improvement, and implementation; patient organisations influence accountability, awareness, and equity. No single stakeholder can close the Implementation Chasm alone. Successful implementation requires coordinated action across the entire healthcare ecosystem.
The Future of the Chasm
Emerging technologies – including artificial intelligence, teleophthalmology, home monitoring systems, and future home OCT platforms – may help narrow elements of the Implementation Chasm. Yet these innovations themselves require implementation. The chasm may evolve, but it is unlikely to disappear entirely. The future question is not whether implementation matters; it is whether healthcare systems can implement innovation as rapidly as science can create it.
Conclusion
The future challenge of AMD is not solely scientific. It is also organisational, operational, economic, and societal. The Implementation Chasm provides a framework for understanding why effective innovations sometimes fail to achieve their full potential. Closing this gap requires governance, workforce development, infrastructure, financing, and equitable delivery systems. Ultimately, the value of innovation is determined not only by what medicine can invent, but also by what healthcare systems can successfully deliver. For every month the Implementation Chasm persists, patients may lose vision that cannot be restored. Closing this gap is not merely an administrative objective – it is a clinical, societal, and moral imperative.
Artificial Intelligence and the Future of AMD Care
From Early Detection to Intelligent Vision Systems
Introduction
The AI question begins in the clinic, not the conference hall. In a busy retina service, OCT scans arrive faster than they can be reviewed, referrals need triage, follow-up intervals stretch, and clinicians carry the risk of missing the patient who should have been seen sooner. AI matters because of that pressure. Not as magic. Not as replacement. As a possible way to make a strained system safer, faster, and more consistent.
Artificial Intelligence (AI) is increasingly transforming healthcare. In ophthalmology, AI has emerged as one of the most promising technological developments of the twenty-first century. Advances in machine learning, deep learning, computer vision, and large-scale image analysis are creating new opportunities for disease detection, risk prediction, workflow optimisation, and healthcare delivery.
AMD is one of the areas where these technologies may most clearly influence future clinical practice. The burden is growing. Imaging volumes are expanding. Workforce pressure is real. New therapies add complexity. AI therefore has a strong case — not only as an efficiency tool, but as a possible route from reactive care toward more proactive, predictive, and personalised models of vision care.
Yet the pace of real-world AI implementation often lags behind technical progress. A model can perform well in a dataset and still fail in a clinic. Who validates the algorithm in older adults, minority populations, low-resource settings, and real-world image quality? Who notices when performance drifts? As discussed in the Implementation Chasm chapter, innovation alone does not guarantee adoption. The value of AI will depend on integration, governance, equity, and trust.
Why AMD Is Well Suited for Artificial Intelligence
Several characteristics make AMD particularly amenable to AI applications:
– Imaging-Rich Disease: Modern AMD care relies heavily on OCT, OCTA, fundus photography, and fundus autofluorescence – all generating large volumes of structured visual data.
– High Disease Burden: The growing prevalence of AMD creates increasing demand for diagnostic and monitoring services.
– Chronic Disease Management: AMD frequently requires monitoring over many years, creating opportunities for automated surveillance, risk stratification, and personalised follow-up.
– Workforce Constraints: As discussed in Workforce Mathematics and the Vision-Care Capacity Gap, demand may outpace workforce growth. AI may therefore function as a capacity multiplier rather than merely a diagnostic tool.
Landmark Studies in AI and AMD
Several landmark studies have demonstrated the transformative potential of AI in retinal care. One of the most influential milestones was the collaboration between Moorfields Eye Hospital, the UCL Institute of Ophthalmology, and DeepMind. In 2018, De Fauw and colleagues published a deep-learning system capable of analysing OCT scans and generating referral recommendations across more than fifty retinal diseases, including AMD. The study demonstrated expert-level diagnostic performance and established AI-assisted OCT interpretation as a realistic clinical possibility [22,45].
Yim and colleagues later demonstrated that deep-learning algorithms could predict future conversion to neovascular AMD in fellow eyes before clinical onset [23]. That was a meaningful advance because it suggested that AI could move beyond diagnosis towards prediction. More recently, investigators have explored AI systems capable of forecasting Geographic Atrophy progression, lesion growth rates, future visual outcomes, and trial-enrichment or recruitment workflows [24,46]. The direction of travel is clear: AI may help clinicians anticipate disease trajectories before irreversible vision loss occurs.
AI for Early Detection
One of the most promising applications of AI is earlier disease detection. Deep-learning systems have demonstrated the ability to identify retinal abnormalities from fundus photographs and OCT scans with high accuracy. Several AMD-related systems have reported area-under-the-curve values exceeding 0.90 for detecting clinically significant retinal pathology. Potential benefits include earlier diagnosis, faster referral pathways, reduced diagnostic delays, improved access to specialist expertise, and more efficient triage systems. Earlier detection may be especially important in identifying patients at increased risk of progression towards advanced AMD.
AI and Risk Prediction
Future AMD care may increasingly focus on prediction rather than reaction. AI systems are being developed to identify imaging biomarkers associated with disease progression, including risk of progression from early to late AMD, GA expansion rates, risk of neovascular conversion, functional decline prediction, and treatment-response forecasting. The goal is not simply to identify disease – it is to anticipate disease trajectories before vision is lost. Such approaches may support more personalised care pathways, targeted monitoring schedules, and more efficient allocation of healthcare resources.
AI and Geographic Atrophy
Geographic Atrophy represents one of the most important future applications of AI in retinal care. AI-assisted image analysis may help detect early atrophic changes, quantify lesion size on OCT, measure progression rates, identify high-risk patients, predict future lesion expansion, and monitor treatment response [24,30]. As disease-modifying therapies become more widely available, demand for accurate monitoring is likely to increase substantially. However, as of 2026, no AI platform has received widespread regulatory approval specifically for predicting GA progression or directing treatment decisions. Most systems remain in developmental, validation, or implementation phases. This distinction is important because scientific promise does not automatically translate into routine clinical use.
AI as a Workforce Multiplier
Artificial intelligence should not be treated as a replacement for clinicians. Its more realistic value is as a workforce multiplier. Earlier triage. Faster prioritisation. Fewer unnecessary visits. Better use of specialist time. Preliminary modelling studies suggest that AI-assisted triage can reduce image-grading workload in high-volume retinal services, but the promise is practical only if implementation is safe, validated, and trusted.
The most persuasive use of AI, in my view, will not be the one that replaces clinical judgement, but the one that gives clinicians more time and better information to use judgement well.
Patient Perspective – Mrs. L is a 68-year-old patient with intermediate AMD. During routine community imaging, an AI-assisted OCT system identifies subtle signs of neovascular conversion and automatically prioritises her referral for urgent review. Within days, she receives specialist assessment and treatment. Without AI-supported triage, referral delays might have postponed intervention for weeks or months. In this scenario, the value of AI is preserved vision.
AI and Health-System Economics
Artificial intelligence requires investment in software acquisition, infrastructure development, workflow integration, workforce training, governance frameworks, and ongoing maintenance. AI is not a cost-free solution. However, AI may generate economic value by reducing unnecessary referrals, improving workflow efficiency, optimising workforce utilisation, and supporting earlier disease detection. The long-term value of AI will depend on whether improvements in patient outcomes and service efficiency outweigh implementation costs.
AI and the Implementation Chasm
Artificial intelligence may help reduce elements of the Implementation Chasm by expanding access to specialist expertise, supporting underserved regions, reducing referral delays, increasing diagnostic consistency, improving service efficiency, and supporting workforce sustainability. However, AI itself requires implementation. Deployment depends upon governance, regulation, infrastructure, workforce training, and digital readiness. AI should be viewed as a tool for narrowing implementation gaps rather than eliminating them entirely.
Governance, Safety, and Trust
The successful adoption of AI depends upon trust. Healthcare systems must address clinical validation, bias and fairness, transparency, accountability, data security, and patient consent. Without appropriate governance, AI may create new risks or widen existing inequalities. The future success of AI in AMD will depend not only on technical performance but also on public trust and institutional governance.
Limitations and Risks
Despite considerable promise, AI faces critical limitations: generalisability across different populations, performance variation across imaging devices, real-world performance gaps, algorithmic bias, limited transparency of some models, regulatory uncertainty, and digital exclusion. For example, algorithms trained primarily on images from one OCT platform may perform less effectively when applied to images generated by another device. Similarly, performance observed in carefully curated research datasets may not always be replicated in routine clinical practice. AI may also create a new form of healthcare inequality. AI has the potential both to narrow and widen disparities depending upon how it is implemented. Addressing these challenges requires continuous validation, prospective evaluation, governance oversight, digital-health governance, and equity-focused implementation [53].
Towards Intelligent Vision Systems
The future of AMD care may extend beyond individual algorithms. This work uses the concept of the Intelligent Vision System to describe a coordinated, continuously learning vision-care ecosystem integrating retinal imaging, artificial intelligence, electronic health records, home monitoring technologies, teleophthalmology, predictive analytics, and clinical decision support. The objective is not merely to detect disease – it is to anticipate risk, support clinicians, optimise resources, improve access, and strengthen health-system resilience.
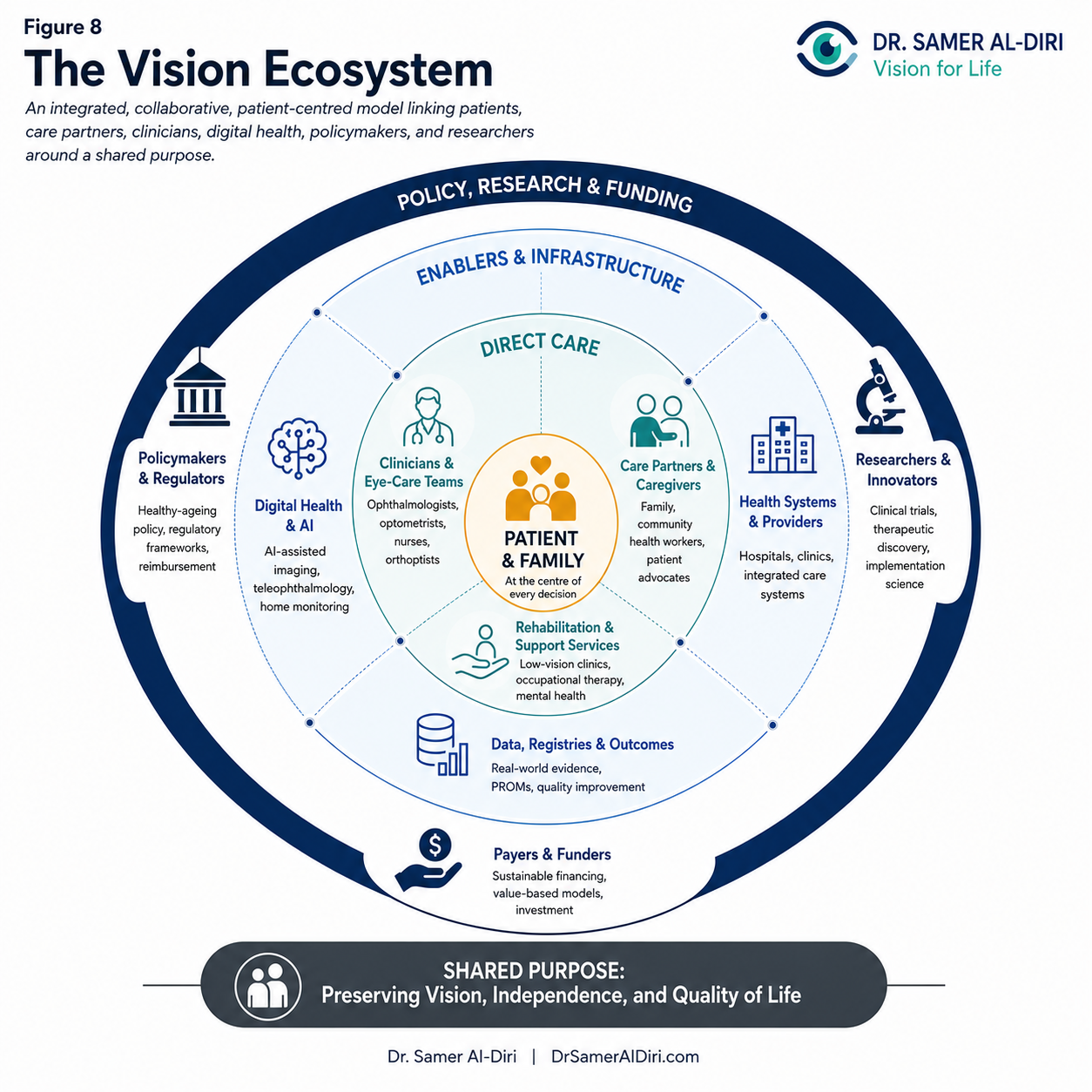
Figure 8. The Vision Ecosystem: an integrated, collaborative, patient-centred model linking patients, care partners, clinicians, digital health, policymakers, researchers, payers, funders, and health systems around a shared purpose.
In this model, AI becomes one component of a broader intelligent care system rather than a standalone technology.
Home Monitoring and the Future of Care
Future AMD care may increasingly extend beyond traditional clinic walls. Emerging technologies include home visual-function monitoring, smartphone-based assessment tools, home OCT platforms, and remote patient-monitoring systems. Combined with artificial intelligence, these approaches may facilitate earlier detection of disease progression while reducing pressure on healthcare facilities. Such technologies have the potential to support more proactive and patient-centred models of care.
Future Directions
Several developments are likely to shape the next decade of AMD care: increasing AI integration into routine practice, expansion of home monitoring technologies, improved predictive analytics, personalised risk-based care pathways, greater use of digital-health platforms, AI-assisted GA monitoring, and Intelligent Vision Systems operating at population scale. These advances may fundamentally reshape how AMD is detected, monitored, and managed.
Conclusion
Artificial intelligence represents one of the most important opportunities for future AMD care. Its greatest contribution may not be replacing clinicians but augmenting healthcare systems, improving efficiency, supporting earlier detection, and helping address workforce and implementation challenges. When combined with strong governance, workforce development, and sustainable health-system planning, AI has the potential to become a major enabler of future-ready vision care. The future of AMD care may depend not only on new therapies, but also on the emergence of intelligent, equitable, and sustainable vision systems capable of delivering those therapies at scale.
From Reactive Care to Future-Ready Vision Systems
Strategic Priorities for Sustainable AMD Care in the Twenty-First Century
From Principle to Delivery
Introduction
The future burden of age-related macular degeneration will not be determined by biology alone. Biology matters, of course. But outcomes will also depend on workforce capacity, financing, digital readiness, public policy, and the ability of health systems to convert scientific advances into fair, timely care.
Throughout this work, AMD has been presented not merely as a retinal disease but as a broader challenge of healthy ageing, health-system sustainability, and healthcare transformation. The emergence of disease-modifying therapies for GA, advances in AI, increasing demands on retinal services, and growing population longevity collectively create both unprecedented opportunities and substantial challenges.
Traditional models of AMD care were largely designed for a different era – an era of shorter life expectancy, fewer therapeutic options, lower imaging demand, and more limited expectations. The coming decades will require a different approach. Healthcare systems must prepare not only for more patients but also for more complex care pathways, higher expectations, and greater pressure on workforce and infrastructure. The challenge is not simply discovering better treatments – it is building healthcare systems capable of delivering those treatments effectively, equitably, and sustainably at scale.
Strategic Priority 1 – Earlier Detection and Risk-Based Prevention
The greatest opportunity in AMD care may occur before advanced disease develops. Future systems should emphasise prevention, early identification, and risk-based monitoring. Priority actions include public awareness campaigns, smoking cessation programmes, cardiovascular risk-factor optimisation, earlier retinal imaging, AI-supported risk stratification, and structured surveillance pathways.
Illustrative Goal: Reduce late-stage AMD diagnosis by 20% over the next decade through improved awareness and earlier detection initiatives.
Strategic Priority 2 – Building Workforce Capacity Before the Crisis
Workforce planning should be viewed as a strategic investment. As demonstrated through Workforce Mathematics and the Vision-Care Capacity Gap, future demand may substantially exceed workforce growth unless action is taken proactively. Priority actions include expansion of ophthalmology training programmes, increased retina-specialist training capacity, advanced allied-health roles, optometrist-supported pathways, nurse-led services, and long-term workforce forecasting. Retina-specialist training frequently requires 5-7 years following medical qualification. Healthcare systems that delay workforce investment today may experience shortages for many years.
Illustrative Goal: Increase retina-care workforce capacity by 25% over the next ten years in regions facing projected demand growth.
Strategic Priority 3 – Developing AI-Enabled Vision Systems
Artificial intelligence should be deployed as part of integrated care systems rather than isolated technological solutions. Priority actions include AI-assisted image interpretation, automated triage, predictive analytics, clinical decision support, home monitoring integration, and teleophthalmology expansion.
Illustrative Goal: Implement AI-supported triage pathways across major retinal centres by 2030.
Strategic Priority 4 – Preparing for the Geographic Atrophy Transition Era
The emergence of disease-modifying therapies for GA marks one of the most important transitions in modern retinal care. Healthcare systems should proactively address patient identification pathways, treatment eligibility frameworks, injection-clinic capacity, imaging infrastructure, outcome monitoring, and reimbursement planning. Failure to prepare may widen the Implementation Chasm.
Illustrative Goal: Establish dedicated GA treatment pathways within major retinal services over the next 2-5 years.
Strategic Priority 5 – Reducing the Implementation Chasm
Innovation without implementation delivers limited population benefit. Priority actions include early implementation planning, regulatory alignment, reimbursement readiness, workforce preparation, infrastructure investment, and real-world evidence generation. Closing the Implementation Chasm may generate population-level benefits comparable in importance to some therapeutic advances.
Illustrative Goal: Reduce the average time between regulatory approval and routine clinical implementation by 50% over the next decade.
Strategic Priority 6 – Embedding Equity into Vision Care
Future innovation must benefit all populations. Priority actions include rural service expansion, mobile eye-care programmes, teleophthalmology, financial-access support, digital-inclusion initiatives, and strengthened services for underserved populations. In lower-resource settings, teleophthalmology, task-shifting, and community-based screening may provide greater immediate benefit than highly specialised infrastructure.
Illustrative Goal: Reduce regional disparities in access to retinal care by at least 30% over the next decade.
Patient Perspective: For patients, a future-ready system means rapid diagnosis, convenient treatment, accessible monitoring, and preserved independence – not simply improved imaging metrics or slower lesion growth.
Strategic Priority 7 – Strengthening Vision-System Resilience
Defining Vision-System Resilience: Vision-System Resilience refers to the ability of a vision-care system to anticipate, absorb, adapt to, and recover from demographic, technological, workforce, financial, and public-health pressures while maintaining equitable access to high-quality eye care. Resilient systems are characterised by workforce flexibility, digital readiness, sustainable financing, strong governance, adaptive service models, and capacity for innovation.
The COVID-19 pandemic provided a powerful illustration. Some healthcare systems rapidly deployed teleophthalmology, community-based monitoring, and alternative care pathways to maintain essential retinal services. Others experienced substantial disruption. Future systems must be designed not only for stability but also for adaptability.
Strategic Priority 8 – Sustainable Financing and Investment
None of the previous priorities can be achieved without sustainable financing. Workforce expansion, GA services, AI deployment, digital infrastructure, home monitoring, and equity initiatives all require investment. Potential financing approaches include value-based reimbursement models, outcome-based payment systems, public-private partnerships, strategic infrastructure investment, reallocation from low-value to high-value care, and long-term prevention-focused funding. Healthcare systems should increasingly view vision preservation as an investment in healthy ageing rather than solely a healthcare expenditure.
Illustrative Goal: Develop financing models that reward long-term patient outcomes rather than service volume alone.
Strategic Priority 9 – Measuring Success Differently
Traditional healthcare metrics frequently focus on activity (number of visits, OCT scans, injections, waiting times). While important, these measures provide only a partial picture. Future AMD care should increasingly evaluate outcomes that matter most to patients and societies: independence preserved, reading ability maintained, mobility preserved, quality of life, vision years preserved, equity outcomes, and patient-reported outcomes. Healthcare systems should ultimately be judged not only by what they deliver, but by what they preserve.
Patient Illustration: For Mr. K, a 70-year-old with intermediate AMD, a future-ready vision system might include community OCT screening, AI-assisted risk identification, rapid specialist review, timely intervention, home monitoring, and preserved reading vision. Success would be measured by the independence retained, not the number of appointments attended.
Priority Implementation Timeline
Immediate Priorities (0-2 Years): GA service preparation, regulatory and reimbursement planning, initial AI readiness assessments, workforce forecasting.
Short-Term Priorities (2-5 Years): Workforce expansion programmes, AI-supported triage deployment, teleophthalmology scaling, equity initiatives.
Medium-Term Priorities (5-10 Years): Intelligent Vision Systems integration, home-monitoring expansion, outcome-based reimbursement models, Vision-System Resilience frameworks.
Long-Term Priorities (10+ Years): Equitable access across all regions, fully integrated intelligent retinal-care ecosystems, sustainable population-scale AMD management.

Figure 9. The Sustainable Vision Strategy: a long-term plan to move from reactive care toward preventive, coordinated, digitally enabled, equitable, and accountable vision systems.
Conclusion
The future challenge of AMD is not simply discovering better treatments. It is building healthcare systems capable of delivering those treatments to the people who need them. Future-ready vision systems will require earlier detection, stronger workforce planning, intelligent use of artificial intelligence, equitable access, implementation excellence, sustainable financing, and resilient healthcare infrastructure. The healthcare systems that begin preparing today will be best positioned to meet the demands of tomorrow. In an era of unprecedented longevity, preserving vision increasingly means preserving independence, participation, wellbeing, and healthy ageing itself. The future of AMD care is therefore a societal, strategic, economic, and healthcare-transformation imperative.
The Future of AMD Care
Seven Forecasts for the Next Decade and Beyond
Reading the Forecasts
Introduction
Any forecast can be upended by a failed trial, a reimbursement decision, a workforce crisis, a recession, or a pandemic. That does not make planning pointless. It makes humility essential.
What follows should be read as informed directions — signposts, not destinations. They are offered to stimulate preparation, not to pretend that the future is already known.
The central proposition remains unchanged: the future challenge is not simply discovering better treatments – it is ensuring that ageing societies possess the workforce, infrastructure, governance, financing, and resilience required to deliver those treatments effectively, equitably, and sustainably.
Forecast 1 – AMD Becomes a Major Healthy-Ageing Policy Priority
– Confidence Level: High
– Time Horizon: 2030-2040
One plausible scenario is that by the mid-2030s, several OECD countries will have incorporated vision-preservation metrics into national healthy-ageing frameworks [39]. If that happens, AMD will be recognised not only as an ophthalmic condition but as a strategic determinant of independence, wellbeing, and social participation.
Forecast 2 – Artificial Intelligence Becomes Embedded Throughout AMD Care Pathways
– Confidence Level: High
– Time Horizon: 2028-2035
AI may cease to feel like a novelty in advanced retinal services. It is likely to become increasingly routine in image interpretation, risk prediction, referral triage, and monitoring. Many newly installed OCT platforms may include AI-assisted analysis within the next decade. Even then, AI should augment — not replace — clinical judgement.
Forecast 3 – Home Monitoring Becomes Mainstream
– Confidence Level: Moderate
– Time Horizon: 2030-2040
Home OCT, digital symptom tracking, and remote visual function tests may be used by a growing minority of stable AMD patients during the 2030s, with higher adoption in technologically mature systems. These tools could reduce unnecessary clinic visits, improve convenience, and enable earlier detection of progression. But home monitoring is elegant only if patients can access the devices, broadband, training, and support required to use them.
Forecast 4 – Geographic Atrophy Treatment Demand Expands Substantially
– Confidence Level: High
– Time Horizon: 2028-2035
As complement inhibitors gain regulatory approvals in more countries — or become available through trials and selected access pathways — the number of patients seeking assessment is likely to rise substantially. This may place major pressure on retina workforces, imaging services, and healthcare budgets.
Forecast 5 – Workforce Shortages Become the Dominant Bottleneck
– Confidence Level: High
– Time Horizon: 2028-2040
If current demand trends continue, retina specialist consultations, procedures, and imaging reviews may outstrip workforce growth in many high-income countries during the next decade, even with moderate task-shifting. Without proactive planning, access to GA therapies and routine AMD monitoring may become increasingly inequitable.
Forecast 6 – Regenerative Medicine Enters Clinical Reality for GA
– Confidence Level: Moderate
– Time Horizon: 2035-2045
It is plausible that one or more cell-based or gene-based therapies will reach regulatory approval for selected GA or AMD populations, offering the possibility of durable disease-modifying or restorative effects. Initial indications are likely to be narrow, possibly limited to highly selected patients, specific disease phenotypes, or carefully defined stages.
Forecast 7 – Vision Preservation Is Recognised Globally as a Pillar of Healthy Ageing
– Confidence Level: Moderate-High
– Time Horizon: 2030-2040
The World Health Organization, OECD, and major national ageing agencies may increasingly include vision-related indicators in healthy-ageing indices [1,37–40]. Vision preservation could become a more visible part of broader health and social policy if ageing strategies move beyond survival alone toward function, independence, and participation.
Future Patient Scenario: AMD Care in 2035
Imagine Mrs. Chen, a 75-year-old retired teacher in 2035. A community OCT scan is analysed by an AI-enabled vision platform. Her progression risk is flagged, and specialist review is arranged within days rather than months. Home monitoring then confirms stability between visits. Imaging biomarkers guide treatment decisions. A digital care coordinator helps with appointments. None of this is science fiction, but none of it is inevitable either. The goal is not merely preventing blindness. It is preserving reading, independence, social participation, and quality of life.
Potential Disruptors
Potential disruptors include failed gene-therapy programmes, unexpected safety concerns, economic recessions, workforce crises, regulatory fragmentation, AI reimbursement failures, cybersecurity disruptions, and future pandemics affecting healthcare delivery.
Forecast Summary
By 2030:
– Structured GA pathways may be established in many advanced systems.
– AI-assisted retinal imaging may become increasingly routine.
– Home monitoring may expand in selected populations.
– Patient-reported outcomes may gain greater influence in service evaluation.
By 2035:
– Vision metrics may be incorporated into healthy-ageing strategies in multiple countries.
– Workforce shortages are likely to become a major strategic concern.
– The Structure–Function Challenge is likely to remain a central policy debate.
– Regenerative medicine may enter late-stage trials for selected GA populations.
By 2040:
– AMD prevalence may approach 290 million globally by 2040, with future burden continuing to rise as populations age.
– Home monitoring could expand substantially in technologically mature systems.
– Intelligent vision-system models may become integrated into routine care pathways.
– Equity may emerge as a principal determinant of population-level outcomes.
Executive Recommendations for Health-System Leaders and Policymakers
Ten Strategic Actions for Sustainable AMD Care in Ageing Societies
Why This Matters Now
Age-related macular degeneration is entering a period of unprecedented transformation. Population ageing is increasing demand for retinal services. Disease-modifying therapies for GA are creating new treatment opportunities and new service pressures. Artificial intelligence is reshaping diagnostic pathways. At the same time, workforce shortages, implementation barriers, inequities in access, and financial constraints threaten the ability of healthcare systems to deliver these advances at scale.
The evidence presented throughout this work suggests that the future success of AMD care will depend not only on scientific innovation but also on health-system readiness. The recommendations that follow are derived directly from the strategic frameworks developed in this work. Together, they provide a practical roadmap for policymakers, healthcare leaders, regulators, professional societies, and healthcare systems seeking to prepare for the coming decades of AMD care.
Evidence-Grading Framework
To support transparency, the recommendations presented in this chapter are accompanied by evidence-grading labels adapted for a flagship policy and strategy publication rather than a formal clinical guideline.
| Evidence Grade | Interpretation |
| High | Supported by multiple randomised controlled trials, systematic reviews, meta-analyses, high-quality population studies, or well-established international guidance. |
| Moderate | Supported by observational studies, implementation research, health-system modelling, or consistent expert consensus, with limited randomised evidence. |
| Low | Supported primarily by emerging evidence, conceptual frameworks, expert opinion, or illustrative modelling requiring further validation. |
Readers should note that some recommendations address health-system design, workforce planning, implementation science, and future-service models. In these areas, randomised controlled trial evidence may be unavailable or inappropriate; therefore, evidence grading reflects the nature of the available evidence rather than the importance of the recommendation.
Recommendation 1 – Integrate Vision Preservation into Healthy Ageing Policy [Moderate]
Vision loss is often treated as a specialist issue until it quietly removes independence, confidence, and social participation from an older person’s life.
The Challenge: Vision remains underrepresented in many national healthy-ageing strategies despite strong evidence linking visual function to independence, mobility, social participation, wellbeing, cognitive health, and quality of life.
Strategic Action: National healthy-ageing strategies should explicitly incorporate vision preservation as a core policy objective. Governments should include vision indicators within national frameworks by 2030, introduce population-level monitoring, integrate vision screening into programmes, and develop cross-sector collaboration.
Lead Stakeholders: Ministries of Health, National Healthy Ageing Programmes, Public Health Agencies, Ophthalmology Societies, Ageing Organisations.
Illustrative Indicators of Progress: Vision metrics incorporated by 2030; 20% increase in AMD risk factor awareness by 2035; 15% reduction in preventable vision-related functional impairment by 2040.
Relevant lens: The Ageing Vision System.
Recommendation 2 – Fund Workforce Expansion Before Capacity Gaps Become Critical [High]
I have seen clinics where the injection list runs late and new patients wait too long for a first assessment. That is what workforce mathematics looks like in practice.
The Challenge: Workforce Mathematics demonstrates that demand for AMD care is increasing more rapidly than workforce capacity. GA therapies, expanding imaging, and population ageing will widen the Vision-Care Capacity Gap.
Strategic Action: Increase ophthalmology training positions by at least 25% by 2030; expand retina fellowship positions by 30% by 2035; implement nurse-led injection clinics and optometrist-led monitoring within 5 years; establish national workforce forecasting models.
Lead Stakeholders: Ministries of Health, Workforce Planning Agencies, Royal Colleges, Academic Institutions.
Illustrative Indicators of Progress: Retina workforce capacity increased by 25% by 2035; vacancy rates below 5%; waiting times reduced by 30%; workforce forecasts updated every 3 years.
Relevant lens: Workforce Mathematics; Vision-Care Capacity Gap.
Recommendation 3 – Prepare National Geographic Atrophy Care Pathways [Moderate]
GA care cannot be improvised after therapies arrive. Patients need clear pathways before the bottleneck becomes visible.
The Challenge: The Geographic Atrophy Transition Era has begun. Many healthcare systems remain unprepared for the service demands associated with disease-modifying therapies.
Strategic Action: Establish national GA clinical pathways by 2030; create standardised eligibility criteria and treatment protocols; expand injection-clinic and imaging capacity; develop GA outcome registries.
Lead Stakeholders: Health Ministries, Regulatory Agencies, Retina Societies, Hospital Networks, Payers.
Illustrative Indicators of Progress: National GA pathways implemented by 2030; treatment waiting times below 4 weeks from eligibility confirmation; registry coverage exceeding 80% of treated patients; annual outcome reporting.
Relevant lens: Geographic Atrophy Transition Era.
Recommendation 4 – Reduce the Implementation Chasm Through Early Planning [High]
A treatment that exists but cannot be accessed is not a solution for the patient sitting in front of us.
The Challenge: Scientific innovation frequently reaches regulatory approval before healthcare systems are prepared to deliver it. This gap limits population-level benefit.
Strategic Action: Require implementation plans alongside major therapeutic approvals; integrate workforce, financing, and infrastructure planning into adoption pathways; establish implementation taskforces; use real-world evidence to evaluate barriers.
Lead Stakeholders: Regulators, Health Technology Assessment Bodies, Health Ministries, Healthcare Executives, Clinical Leaders.
Illustrative Indicators of Progress: Reduction of approval-to-implementation delays by 50% by 2035; national implementation plans for all major AMD innovations; annual reporting on access disparities.
Relevant lens: The Implementation Chasm.
Recommendation 5 – Invest in AI-Enabled Vision Systems with Strong Governance [Moderate]
AI can help, but only if patients and clinicians can trust how it was trained, validated, monitored, and governed.
The Challenge: AI offers substantial opportunities to improve efficiency, capacity, and access. However, poorly governed implementation risks bias, inequity, and loss of trust.
Strategic Action: Develop national AI governance frameworks for ophthalmology by 2030; deploy AI-supported OCT triage and referral systems; ensure prospective validation across diverse populations; establish mandatory monitoring of safety, performance, and equity.
Lead Stakeholders: Health Ministries, Digital Health Authorities, Regulators, Healthcare Organisations, Technology Developers.
Illustrative Indicators of Progress: AI-assisted triage available in ≥80% of major retinal centres by 2035; reduction in unnecessary referrals by 30%; demonstrated equity monitoring in all AI-enabled pathways.
Relevant lens: Intelligent Vision Systems.
Recommendation 6 – Expand Home Monitoring and Teleophthalmology [Moderate]
Home monitoring may reduce travel and clinic pressure, but it must work for older adults living with real digital, social, and practical constraints.
The Challenge: Traditional hospital-centred monitoring models may become unsustainable as AMD prevalence rises.
Strategic Action: Pilot home OCT and remote monitoring programmes by 2030; expand teleophthalmology networks in rural and underserved regions; integrate home monitoring data into electronic health records; develop reimbursement pathways for virtual care.
Lead Stakeholders: Health Ministries, Health Insurers, Hospital Systems, Digital Health Providers.
Illustrative Indicators of Progress: Progressive expansion of home monitoring in suitable patient groups, with measurable adoption targets adapted to local digital maturity, reimbursement models, and patient-support capacity; reduced rural access disparities; and fewer unnecessary follow-up visits.
Relevant lens: The Sustainable Vision Care Framework.
Recommendation 7 – Establish National AMD Registries and Outcome Frameworks [High]
Without real-world data, health systems are left guessing which innovations improve lives and which merely increase activity.
The Challenge: Many healthcare systems lack robust longitudinal data regarding AMD outcomes, service performance, patient-reported outcomes, and implementation effectiveness.
Strategic Action: Create national AMD registries by 2030; include patient-reported outcome measures (PROMs) and quality-of-life metrics; link registry data to workforce planning, service design, and reimbursement; promote international benchmarking.
Lead Stakeholders: Governments, Professional Societies, Academic Centres, Healthcare Providers.
Illustrative Indicators of Progress: Registry coverage exceeding 80% of treated patients; routine collection of PROMs; annual national AMD outcome reports.
Relevant lens: Measuring Success Differently.
Recommendation 8 – Embed Equity into Every AMD Innovation Strategy [Moderate]
Innovation can widen inequality if the first beneficiaries are only those already closest to specialist care.
The Challenge: Without deliberate intervention, innovations may widen disparities between urban/rural populations, high-income/low-income regions, and digitally connected/excluded communities.
Strategic Action: Establish equity impact assessments for all major AMD programmes; expand mobile retinal services and community screening; develop targeted programmes for underserved populations; incorporate equity targets into funding and evaluation.
Lead Stakeholders: Governments, Public Health Agencies, Health Equity Programmes, Community Organisations.
Illustrative Indicators of Progress: Reduction in regional access variation by 30% by 2035; increased service utilisation in underserved populations; annual publication of AMD equity metrics.
Relevant lens: The Sustainable Vision Care Framework.
Recommendation 9 – Strengthen Vision-System Resilience [Low to Moderate]
Retina services need to absorb pressure without quietly sacrificing safety, staff wellbeing, or timely access.
The Challenge: Future AMD services must withstand demographic pressures, workforce shortages, technological disruption, financial constraints, and public-health emergencies.
Strategic Action: Develop Vision-System Resilience strategies by 2030; build digitally enabled service models capable of maintaining care during disruptions; expand community-based service capacity; conduct resilience exercises and scenario planning every 2-3 years.
Lead Stakeholders: Health Ministries, Hospital Systems, Emergency Preparedness Agencies, Clinical Networks.
Illustrative Indicators of Progress: Resilience plans implemented nationally by 2030; maintenance of essential AMD services during major disruptions; annual resilience performance reporting.
Relevant lens: Vision-System Resilience.
Recommendation 10 – Align Financing and Evaluation with Outcomes That Matter [Moderate]
The real question is not only whether a treatment slows a lesion. It is whether people read, move, recognise faces, and remain independent for longer.
The Challenge: Many reimbursement systems reward activity rather than outcomes. Sustainable AMD care requires financing models aligned with patient benefit, independence, and long-term value.
Strategic Action: Pilot outcome-based reimbursement models by 2030; incorporate patient-reported outcomes into funding decisions; support value-based care pathways focused on vision preservation; prioritise investment in interventions that demonstrate long-term functional benefit.
Lead Stakeholders: Governments, Payers, Health Technology Assessment Bodies, Healthcare Providers.
Illustrative Indicators of Progress: Outcome-based payment models implemented in AMD care by 2035; PROMs incorporated into reimbursement decisions; increased investment in prevention, rehabilitation, and vision-preservation programmes.
Relevant lens: Vision Years Preserved; The Sustainable Vision Care Framework.
Final Policy Message
The future success of AMD care will depend not only on scientific discovery but also on the willingness of healthcare systems to act proactively. The recommendations presented above provide a practical framework for translating innovation into sustainable population-level benefit. Healthcare systems that begin preparing now will be best positioned to meet the challenges of ageing societies, the growing burden of AMD, and the emerging realities of the Geographic Atrophy Transition Era. The future of AMD care will ultimately be determined not by what medicine can invent, but by what healthcare systems can successfully deliver.
Adapting Sustainable Vision Care Across Diverse Health‑System Contexts
The strategic priorities and recommendations draw heavily on evidence and implementation experience from health systems with established ophthalmology workforces, retinal imaging infrastructure, and regulatory pathways for advanced therapies. That is not the whole world. Many low‑ and middle‑income countries (LMICs) and limited‑resource settings begin from very different starting points: ophthalmology workforces may be severely constrained, particularly outside major urban centres; OCT machines may be absent beyond a few tertiary hospitals; and disease‑modifying therapies for GA may not yet be accessible or affordable.
Population ageing is accelerating most rapidly in many LMICs, so the future burden of AMD will not remain concentrated in high-income countries. The same demographic forces driving AMD prevalence in Europe, North America, and East Asia are now reshaping eye-health needs across Africa, South Asia, and the Pacific.
Sustainable vision care is ultimately an equity challenge: preserving sight should not depend solely on geography, income, or proximity to specialist services. The principles are shared — prevention, early detection, feasible treatment, rehabilitation, workforce development, and resilience — but the pathway changes. In many settings, the first step is not a new therapy. It is awareness, referral, basic imaging, trained personnel, and support for families.
Prevention and risk reduction as the highest‑return investment
Where advanced therapies are not available, preventing AMD and delaying progression becomes the most cost‑effective strategy. Priorities include:
– Public awareness campaigns on smoking cessation and cardiovascular risk reduction.
– Integration of basic vision screening into primary care and non‑communicable disease programmes (diabetes, hypertension).
– Low‑cost nutritional advice (dark green leafy vegetables) aligned with AREDS2 principles [36].
Task‑shifting and non‑physician workforce development
Retina specialists are scarce, but optometrists, ophthalmic nurses, and community health workers can be trained to:
– Identify AMD features using simplified protocols (drusen, pigment changes, subretinal fluid).
– Perform fundus photography using low‑cost or smartphone‑based devices.
– Refer high‑risk patients to a regional hub where OCT and specialist review are available (even if only monthly).
Artificial intelligence as a force multiplier
In settings where specialist retina expertise is extremely limited, AI may have greater relative value than in well‑resourced systems. Specifically:
– AI‑assisted interpretation of fundus photographs or OCT images may help extend specialist expertise across geographically dispersed services and support more efficient triage pathways.
– Automated triage algorithms can prioritise the small number of patients requiring rare in‑person visits.
– Even store‑and‑forward teleophthalmology with AI pre‑screening can reduce unnecessary travel and lost wages for patients.
This aligns directly with the Intelligent Vision System concept discussed earlier: AI does not replace clinicians but democratises access to specialist‑level insight.
Teleophthalmology and Regional Hub‑and‑Spoke Models
Instead of building expensive OCT capacity in every district, sustainable models include:
– One regional centre with OCT, angiography, and injection capability serving a large catchment population through a hub‑and‑spoke network.
– Spoke clinics using portable fundus cameras (or smartphone attachments) with internet transmission to the hub.
– Visiting retina specialist teams that rotate through peripheral sites quarterly.
Low‑vision rehabilitation before, during, and after therapy
For the vast majority of patients with advanced AMD in LMICs, the most impactful intervention is not a complement inhibitor but:
– Simple, low‑cost magnifiers and lighting adjustments.
– Orientation and mobility training delivered by community rehabilitation workers.
– Family caregiver education on maintaining independence and safety.
These services also benefit patients receiving anti‑VEGF or future GA therapies, who still experience irreversible photoreceptor loss.
Research, advocacy, and affordable innovation
International partners, NGOs, and philanthropic organisations should prioritise:
– Development and validation of low‑cost, solar‑powered, heat‑stable OCT devices suitable for tropical climates.
– Price negotiations and voluntary licensing for future GA therapies, biosimilars, and AI software.
– Implementation research conducted in LMICs, not imported from high‑income settings – including studies on what works for rural, low‑literacy, and culturally diverse populations.
What I Have Learned Across Health Systems
Working across the United Kingdom, the United Arab Emirates, humanitarian settings, and the South Pacific has taught me a simple lesson: the principles may be shared, but the order of implementation changes. In one system, the priority may be reducing injection backlogs. In another, it may be bringing OCT within reach. Elsewhere, the first step may be training a non-physician workforce to recognise disease early enough to refer. Sustainable vision care starts where the system is. It does not wait for ideal conditions.
Conclusion
No single AMD strategy will fit every country. Ignoring the diversity of health-system contexts would make any global discussion feel artificial. The six adaptations above are offered as a starting point for policymakers and clinical leaders in LMICs and limited-resource settings. The broad principles remain useful; local leadership, innovation, financing, culture, and workforce reality determine implementation.
Call to Action
Preparing for the Ageing Vision Century
Imagine a woman in her late seventies who can no longer read her grandson’s handwritten note, not because she lacks the will, but because her central vision has faded. That quiet loss is repeated millions of times over. Population ageing turns those individual losses into a health-system responsibility.
People are living longer than any previous generation. That is one of the great achievements of modern medicine, public health, education, and socioeconomic development. It also changes the task before us: health systems built around younger populations and episodic illness must adapt to the chronic realities of ageing societies.
The phrase Ageing Vision Century is used here to describe a period in which population ageing makes vision preservation one of the defining health, social, and economic priorities of the twenty-first century.
Age-related macular degeneration sits at the centre of this transformation. For decades, AMD was viewed principally as a retinal disease affecting older adults. Today, it is clear that AMD represents something much larger. It is a public-health challenge, a healthy-ageing challenge, a workforce challenge, a health-system challenge, and a test case for the future sustainability of chronic disease care.
The consequences of inaction are becoming increasingly visible. Without proactive planning, many healthcare systems may face widening Vision-Care Capacity Gaps, growing workforce shortages, longer waiting times, unequal access to innovation, and expanding disparities in outcomes. Scientific progress alone cannot prevent these pressures. New therapies, advanced imaging, AI, and home-monitoring systems can only improve outcomes when supported by sufficient workforce capacity, effective implementation, sustainable financing, and equitable access.
The Geographic Atrophy Transition Era has already begun. For the first time, disease-modifying therapies offer the possibility of slowing progression in a condition previously considered untreatable. However, the ultimate success of this transition will not be determined solely by regulatory approvals or clinical-trial outcomes. It will be determined by whether healthcare systems possess the capacity to deliver these innovations to the patients who need them.
The central message is clear: AMD care cannot rely on innovation alone. Healthcare leaders need to prepare workforces before shortages become critical. Policymakers need to integrate vision preservation into healthy-ageing strategies. Regulators and payers need to reduce unnecessary implementation delays. Researchers must keep pursuing therapies that improve outcomes patients can feel. Technology developers must deploy AI responsibly, transparently, and equitably. Professional societies need to support service redesign, education, and workforce development. Together, these choices will determine whether scientific advances become population-level benefit.
The challenge is global. In high-income countries, ageing populations are increasing demand for specialist retinal services. In low- and middle-income countries, workforce shortages and limited infrastructure threaten to widen existing inequalities. Yet despite these differences, the underlying objective remains the same: ensuring that all individuals have access to timely, effective, and sustainable vision care regardless of geography, income, or circumstance.
This work has used several frameworks to support that objective: The Ageing Vision System, The Sustainable Vision Care Framework, Workforce Mathematics, the Vision-Care Capacity Gap, the Geographic Atrophy Transition Era, the Implementation Chasm, Vision-System Resilience, and Intelligent Vision Systems. Although each framework addresses a different dimension of AMD care, all point toward a common conclusion:
The future success of AMD care will depend not only on what medicine can discover, but also on what healthcare systems can deliver.
A Global Goal for 2030
Governments, health ministries, professional societies, researchers, healthcare organisations, patient advocates, and international health institutions should work toward one shared objective:
By 2030, every health system should have a national AMD and healthy-vision strategy with measurable goals for workforce capacity, implementation readiness, equitable access, and patient-centred outcomes.
The coming decade represents a critical window of opportunity. Healthcare systems that prepare early will be best positioned to meet the demands of ageing populations. Those that delay risk widening implementation gaps and avoidable vision loss.
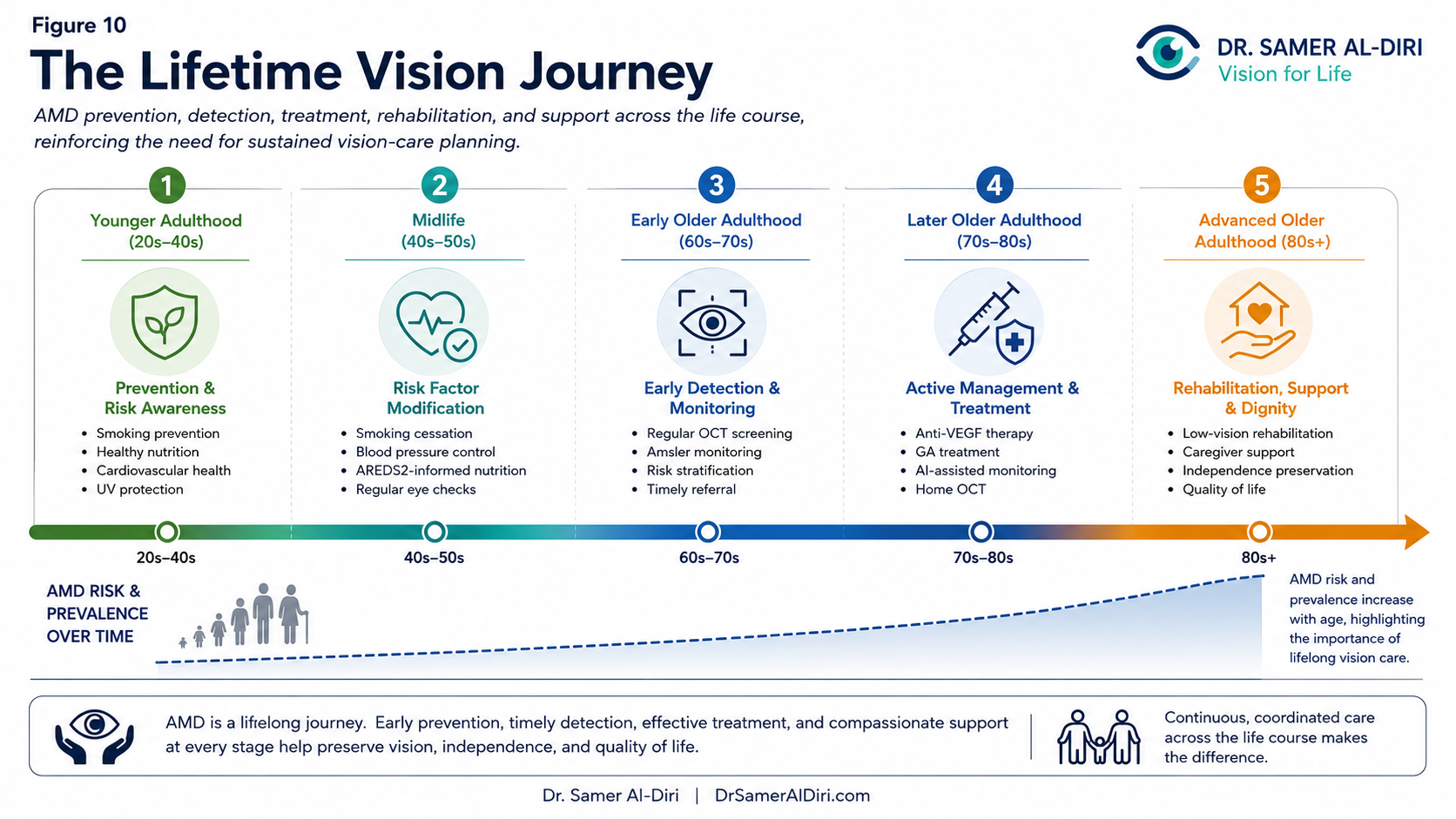
Figure 10. The Lifetime Vision Journey: AMD prevention, detection, treatment, rehabilitation, and support across the life course, reinforcing the need for sustained vision-care planning.
Immediate Imperatives for 2026-2027
Preparation cannot begin in the future. It must begin now. As immediate priorities, healthcare systems should:
– Publish national AMD workforce forecasts and capacity assessments.
– Establish multidisciplinary taskforces for GA implementation planning.
– Integrate vision metrics into healthy-ageing frameworks and national health indicators.
– Launch pilot programmes for home monitoring, teleophthalmology, and AI-assisted retinal care.
– Develop national AMD registries capable of tracking outcomes, equity, and service performance.
– Assess implementation readiness for emerging therapies before approval decisions occur.
These actions represent practical first steps toward sustainable vision care.
Accountability and Measuring Progress
Meaningful change requires accountability. One practical option would be a Global AMD Progress Report, published every three years, to monitor progress in workforce development, implementation readiness, equity, access, patient outcomes, and health-system resilience. Such reporting could help governments, professional societies, researchers, and patient organisations identify areas of success, highlight implementation gaps, and share best practices internationally. The future of AMD care should be measured not only by scientific advances but also by the extent to which those advances reach patients.
Patients and the Public Must Be Part of the Solution
The future of AMD care cannot be shaped solely by governments, healthcare systems, clinicians, or researchers. Patients, families, caregivers, and advocacy organisations must also play a central role. Public awareness remains one of the most underutilised tools in vision preservation. Greater awareness of AMD risk factors, symptoms, treatment options, and the importance of early detection can improve outcomes and strengthen support for policy change. Patients and advocacy organisations should actively encourage policymakers to prioritise vision preservation within healthy-ageing strategies. Their voices are essential in ensuring that healthcare systems remain focused on the outcomes that matter most.
The Opportunity Before Us
Preparing for the Ageing Vision Century requires action today. The decisions made during the next decade will shape the experiences of millions of people living with AMD over the coming generation. Health systems that invest early in workforce capacity, sustainable service models, equitable implementation, digital innovation, and resilient infrastructure will be best positioned to meet future demand.
Ultimately, the goal is not simply to preserve retinal structure, slow lesion growth, or improve healthcare metrics. The goal is to preserve the ability to read, recognise loved ones, maintain independence, participate in society, and live with dignity throughout later life.
Preparing for the Ageing Vision Century is not merely a healthcare priority – it is an investment in healthy ageing itself.
The Ageing Vision Century will be remembered not by the therapies it invents, but by the vision it preserves.
Final Reflection: The Future of Vision in an Ageing World
Age-related macular degeneration is a retinal disease. But it is also more than that. The evidence points to a broader and more urgent framing: AMD is a defining challenge of ageing societies.
The twenty-first century will be remembered for unprecedented longevity. Yet longer lives are only a triumph if they are accompanied by preserved function, independence, dignity, and social participation. Vision is the sensory foundation of almost everything we value in later life: reading, recognising loved ones, moving safely, staying connected, and living autonomously.
The Longevity–Vision Paradox captures the dilemma: the same advances that extend lifespan increase the population at risk of age-related visual impairment. The Ageing Vision System reframes the solution: vision preservation must become a core pillar of healthy ageing, supported by sustainable, equitable, and resilient vision-care systems.
The Geographic Atrophy Transition Era has begun. For the first time, treatments exist that can slow the progression of a previously untreatable condition. But this era is characterised by modest benefits, hard trade-offs, and unresolved questions – the Structure–Function Challenge, safety considerations, workforce constraints, and implementation gaps. Evidence-based hope is the only responsible guide.
The future of AMD care will not be determined solely by what medicine can invent. It will be determined by what healthcare systems can deliver: workforce capacity before crises, AI-enabled efficiency without inequity, home monitoring that respects privacy and access, and financing that rewards outcomes that matter to patients – independence, reading, mobility, and quality of life.
The Sustainable Vision Care Framework, the Vision Dividend, Workforce Mathematics, the Implementation Chasm, and the other concepts discussed here are not academic exercises. They are practical tools for governance. I hope researchers, clinicians, policymakers, and patient advocates will test, challenge, adapt, and improve them. That is how ideas become useful.
If there is one message I would leave with the reader, it is this: preserving sight is not a narrow ophthalmic ambition. It is a way of protecting independence, dignity, memory, work, family life, and the confidence to remain part of the world.
The Ageing Vision Century will not be defined by the therapies we invent. It will be defined by the vision we choose to preserve – in every clinic, every health system, and every ageing society.
The future of vision care will ultimately be judged not by the sophistication of its technologies or the number of therapies available, but by its ability to preserve the capabilities that allow people to live independently, participate fully in society, and age with dignity.
Competing Interests
I have no financial, commercial, institutional, or personal interests that could influence the content of this work. The conclusions are my own, drawn from the evidence as I understand it at the time of writing.
Funding Statement
No external funding was received for the preparation, writing, analysis, or publication of this work. I independently conceived, researched, and developed this work. No funding body had any role in the design, analysis, interpretation, writing, or decision to publish.
Author Biography
Dr. Samer Al-Diri is a Consultant Ophthalmologist and Retina Specialist with professional experience spanning ophthalmology, public health, healthcare management, healthcare transformation, and health-system strengthening.
He completed advanced ophthalmology and retina training through internationally recognised institutions including the Institute of Ophthalmology, University College London, and Moorfields Eye Hospital, London. He also holds a Master of Public Health (Healthcare Planning and Management) with Merit from City, University of London.
His professional experience spans the United Kingdom, the United Arab Emirates, the South Pacific, and humanitarian and health-system settings in the Middle East.
His work focuses on retinal disease, healthy ageing, healthcare transformation, health-system resilience, healthcare governance, artificial intelligence in healthcare, digital health innovation, and sustainable healthcare delivery.
This work was developed to explore the growing intersection between retinal innovation, population ageing, health-system preparedness, healthcare transformation, and the future of sustainable vision care.
Website: https://drsameraldiri.com
Suggested Citation
Al-Diri S. Age-Related Macular Degeneration: Population Ageing, Health-System Impact, Artificial Intelligence, and the Future of Sustainable Vision Care — Preserving Sight in an Ageing World. DrSamerAlDiri.com. Published 23 June 2026. Available at: https://drsameraldiri.com/age-related-macular-degeneration-population-ageing-health-system-impact-artificial-intelligence-and-the-future-of-sustainable-vision-care/
Accessed 23 June 2026.
Open Access Licensing Statement
Open Access Reference Publication. © 2026 Dr. Samer Al-Diri.
This work is distributed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) licence. It may be downloaded and shared for non-commercial purposes with appropriate credit to the author. Modifications, adaptations, or derivative works require written permission.
Licence details: Creative Commons CC BY–NC–ND 4.0
Disclaimer
This material is intended for educational, academic, strategic, and informational purposes only. It reflects my interpretation of the available evidence and should not be treated as individual medical advice, legal advice, policy advice, or professional consultation. I do not endorse any specific commercial product, therapy, organisation, or manufacturer referenced in the publication. Clinical decisions should always be based on individual patient circumstances, professional judgement, current clinical guidelines, and applicable regulatory requirements. Although every effort has been made to ensure accuracy at the time of publication, medical evidence, technologies, regulatory decisions, and treatment pathways may change over time.
Abbreviations
Concise glossary of key abbreviations used throughout this flagship publication.
| Abbreviation | Definition | Abbreviation | Definition |
| AI | Artificial Intelligence | LMICs | Low- and Middle-Income Countries |
| AMD | Age-Related Macular Degeneration | ML | Machine Learning |
| AUC | Area Under the Curve | nAMD | Neovascular Age-Related Macular Degeneration |
| BCVA | Best-Corrected Visual Acuity | NHS | National Health Service |
| C3 | Complement Component 3 | NICE | National Institute for Health and Care Excellence |
| C5 | Complement Component 5 | OCT | Optical Coherence Tomography |
| CC BY-NC-ND 4.0 | Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Licence | OCTA | Optical Coherence Tomography Angiography |
| DL | Deep Learning | OECD | Organisation for Economic Co-operation and Development |
| EMA | European Medicines Agency | PROMs | Patient-Reported Outcome Measures |
| FAF | Fundus Autofluorescence | ROI | Return on Investment |
| FDA | United States Food and Drug Administration | RPE | Retinal Pigment Epithelium |
| FTE | Full-Time Equivalent | UCL | University College London |
| GA | Geographic Atrophy | UK | United Kingdom |
| GBD | Global Burden of Disease | US | United States |
| HTA | Health Technology Assessment | VEGF | Vascular Endothelial Growth Factor |
| ICO | International Council of Ophthalmology | WHO | World Health Organization |
References
1. World Health Organization. World report on vision. Geneva: WHO; 2019.
2. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040. Lancet Glob Health. 2014;2(2):e106-16.
3. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020. Lancet Glob Health. 2017;5(12):e1221-34.
4. GBD 2019 Blindness and Vision Impairment Collaborators. Causes of blindness and vision impairment in 2020 and trends over 30 years. Lancet Glob Health. 2021;9(2):e144-60.
5. United Nations, Department of Economic and Social Affairs. World Population Ageing 2020 Highlights. New York: UN; 2020.
6. Lord SR, Dayhew J, Howland A. Multifocal glasses impair edge-contrast sensitivity and increase the risk of falls in older people. J Am Geriatr Soc. 2002;50(11):1769-75.
7. Marques AP, Ramke J, Cairns J, et al. Global economic productivity losses from vision impairment and blindness. EClinicalMedicine. 2021;35:100852.
8. Dawson SR, Mallen CD, Gouldstone MB, Yarham R, Mansell G. The prevalence of anxiety and depression in people with age-related macular degeneration: a systematic review of observational study data. BMC Ophthalmol. 2014;14:78. doi:10.1186/1471-2415-14-78.
9. Casten RJ, Rovner BW. Depression in age-related macular degeneration. J Vis Impair Blind. 2008;102(10):624-30.
10. Crews JE, Chou CF, Stevens JA, Saaddine JB. Falls among persons with visual impairment in the United States, 2012-2016. JAMA Ophthalmol. 2020;138(5):504-11.
11. Lamoureux EL, Hassell JB, Keeffe JE. Visual impairment and physical functioning in older adults. Ophthalmology. 2004;111(7):1349-54.
12. Binns AM, Bunce C, Dickinson C, Harper RA, Tudor-Edwards R, Woodhouse M, et al. How effective is low vision service provision? A systematic review. Surv Ophthalmol. 2012;57(1):34-65. doi:10.1016/j.survophthal.2011.06.006.
13. Brown MM, Brown GC, Sharma S, et al. Quality of life and caregiver burden associated with age-related macular degeneration. Ophthalmology. 2005;112(6):1077-84.
14. NHS England. Hospital outpatient activity, 2022-23: ophthalmology specialty report. NHS Digital; 2023.
15. Public Health England. Atlas of Variation in Risk Factors and Healthcare for Vision in England: Intravitreal Injection Therapy. London: Public Health England; 2021.
16. Paudel N, Brady L, Stratieva P, et al. Economic burden of late-stage age-related macular degeneration in Bulgaria, Germany, and the US. JAMA Ophthalmol. 2024;142(12):1123-1130. doi:10.1001/jamaophthalmol.2024.4401.
17. Resnikoff S, Lansingh VC, Washburn L, et al. Estimated number of ophthalmologists worldwide. Br J Ophthalmol. 2020;104(4):588-92.
18. Graham R. Facing the crisis in human resources for eye health in sub-Saharan Africa. Community Eye Health. 2017;30(100):85-87. PMID:29483753; PMCID:PMC5820633.
19. US Food and Drug Administration. SYFOVRE (pegcetacoplan injection), for intravitreal use: prescribing information. Silver Spring, MD: FDA; updated 2025.
20. European Medicines Agency. Questions and answers on the refusal of the marketing authorisation for Syfovre (pegcetacoplan). EMA/432931/2024. Amsterdam: EMA; 2024.
21. National Institute for Health and Care Excellence. Pegcetacoplan for treating geographic atrophy [ID4041]. NICE technology appraisal in development: discontinued. GID-TA11351. London: NICE; 2026.
22. De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24(9):1342-50.
23. Yim J, Chopra R, Spitz T, et al. Predicting conversion to wet age-related macular degeneration using deep learning. Nat Med. 2020;26(6):892-9.
24. Reiter GS, Lachinov D, Bühl W, Weigert G, Grechenig C, Mai J, Bogunović H, Schmidt-Erfurth U. A novel management challenge in age-related macular degeneration: artificial intelligence and expert prediction of geographic atrophy. Ophthalmol Retina. 2025 May;9(5):421-430. doi:10.1016/j.oret.2024.10.029. PMID:39522752.
25. Heier JS, Lad EM, Holz FG, Rosenfeld PJ, Guymer RH, Boyer D, et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): two multicentre, randomised, double-masked, sham-controlled, phase 3 trials. Lancet. 2023;402(10411):1434-1448. doi:10.1016/S0140-6736(23)01520-9. PMID:37865470.
26. Khanani AM, Patel SS, Staurenghi G, Dugel PU, Eichenbaum DA, Heier JS, et al.; GATHER2 Trial Investigators. Efficacy and safety of avacincaptad pegol in patients with geographic atrophy (GATHER2): 12-month results from a randomised, double-masked, phase 3 trial. Lancet. 2023;402(10411):1449-1458. doi:10.1016/S0140-6736(23)01583-0. PMID:37696275.
27. Patel SS, Lally DR, Hsu J, Wykoff CC, Eichenbaum D, Heier JS, Jaffe GJ, Westby K, Desai D, Zhu L, Khanani AM. Avacincaptad pegol for geographic atrophy secondary to age-related macular degeneration: 18-month findings from the GATHER1 trial. Eye (Lond). 2023;37(17):3551-3557. doi:10.1038/s41433-023-02497-w. PMID:36964259.
28. US Food and Drug Administration. IZERVAY (avacincaptad pegol intravitreal solution): prescribing information. Silver Spring, MD: FDA; updated 2025.
29. Holz FG, Le Mer Y, Muqit MMK, Hattenbach LO, Cusumano A, Grisanti S, et al. Subretinal photovoltaic implant to restore vision in geographic atrophy due to AMD. N Engl J Med. 2026;394(3):232-242. doi:10.1056/NEJMoa2501396. PMID:41124203.
30. Zhang G, Fu DJ, Liefers B, et al. Clinically relevant deep learning for detection and quantification of geographic atrophy from optical coherence tomography: a model development and external validation study. Lancet Digit Health. 2021;3(10):e665-e675. doi:10.1016/S2589-7500(21)00134-5.
31. Holekamp NM, de Beus AM, Clark WL, Heier JS. Prospective trial of home optical coherence tomography-guided management of treatment-experienced neovascular age-related macular degeneration patients. Retina. 2024;44(10):1714-1731. doi:10.1097/IAE.0000000000004167. PMID:39287534.
32. Khanani AM, Guymer RH, Wykoff CC, Basu K, Eter N, Korobelnik JF, et al.; TENAYA and LUCERNE Investigators. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914-926. doi:10.1016/j.ophtha.2024.02.014. PMID:38382813.
33. Heier JS, Khanani AM, Quezada Ruiz C, Basu K, Ferrone PJ, Brittain C, et al.; TENAYA and LUCERNE Investigators. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729-740. doi:10.1016/S0140-6736(22)00010-1. PMID:35085502.
34. Lanzetta P, Korobelnik JF, Heier JS, Leal S, Holz FG, Clark WL, et al.; PULSAR Investigators. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet. 2024;403(10432):1141-1152. doi:10.1016/S0140-6736(24)00063-1. PMID:38461841.
35. Holekamp NM, Campochiaro PA, Chang MA, Miller D, Pieramici D, Adamis AP, et al. Archway randomized phase 3 trial of the Port Delivery System with ranibizumab for neovascular age-related macular degeneration. Ophthalmology. 2022;129(3):295-307. doi:10.1016/j.ophtha.2021.09.016. PMID:34597713.
36. Chew EY, Clemons TE, SanGiovanni JP, Danis R, Ferris FL 3rd, Elman MJ, et al.; Age-Related Eye Disease Study 2 (AREDS2) Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the AREDS2 randomized clinical trial. JAMA. 2013;309(19):2005-2015. doi:10.1001/jama.2013.4997. PMID:23644932.
37. World Health Organization. World report on ageing and health. Geneva: WHO; 2015.
38. World Health Organization. Integrated people-centred eye care (IPEC). Geneva: WHO; 2020.
39. Organisation for Economic Co-operation and Development. Health at a glance 2023: OECD indicators. Paris: OECD Publishing; 2023.
40. World Bank. Unlocking the Power of Healthy Longevity: Demographic Change, Non-communicable Diseases, and Human Capital. Washington, DC: World Bank; 2024.
41. Vision Loss Expert Group of the Global Burden of Disease Study. Global estimates of vision loss and its causes, 1990-2020. IHME; 2021.
42. Macular Society. Geographic atrophy: patient-reported outcomes and quality of life. London: Macular Society; 2023.
43. Retina International. PRIMA retinal implant: patient information and research summary. Dublin: Retina International; 2025.
44. NHS England. Ophthalmology transformation: workforce and capacity planning. London: NHS England; 2023.
45. Moorfields Eye Hospital NHS Foundation Trust. Moorfields/UCL AI research programme: OCT and AMD progression. London: Moorfields Eye Charity; 2020.
46. UCL Institute of Ophthalmology. AI-supported geographic atrophy trial recruitment. London: UCL; 2024.
47. ClinicalTrials.gov. OCU410 ArMaDa (NCT06018558). National Library of Medicine; 2023.
48. ClinicalTrials.gov. JNJ-81201887 (NCT05811351). National Library of Medicine; 2023.
49. ClinicalTrials.gov. GT005 EXPLORE (NCT04437368). National Library of Medicine; 2020.
50. ClinicalTrials.gov. OpRegen (NCT02286089). National Library of Medicine; 2014.
51. Novartis. Novartis announces decision to discontinue development of GT005. Press release. November 14, 2023.
52. Tzoumas N, Riding G, Williams MA, Steel DHW. Complement inhibitors for age-related macular degeneration. Cochrane Database Syst Rev. 2023;2023(6):CD009300. doi:10.1002/14651858.CD009300.pub3. PMID:37314061.
53. World Health Organization. Digital health and AI guidance. Geneva: WHO; 2024.
54. Ehlers JP, Hu A, Boyer D, et al. ReCLAIM-2: a randomized phase II clinical trial evaluating elamipretide in age-related macular degeneration, geographic atrophy growth, visual function, and ellipsoid zone preservation. Ophthalmol Sci. 2024;5(1):100628. doi:10.1016/j.xops.2024.100628.
55. ClinicalTrials.gov. ReNEW: Phase 3 Study of Efficacy, Safety and Pharmacokinetics of Subcutaneous Injections of Elamipretide in Subjects with Dry Age-Related Macular Degeneration. Identifier: NCT06373731. National Library of Medicine; 2024.
56. ClinicalTrials.gov. Phase 3, Randomized, Placebo-Controlled Study of Tinlarebant to Explore Safety and Efficacy in Geographic Atrophy (PHOENIX). Identifier: NCT05949593. National Library of Medicine; 2023.
57. ClinicalTrials.gov. A Study Investigating the Efficacy and Safety of Intravitreal Injections of Vonaprument (ANX007) in Participants with Geographic Atrophy Secondary to Age-Related Macular Degeneration. Identifier: NCT06510816. National Library of Medicine; 2024.
58. ClinicalTrials.gov. A Study Investigating Subcutaneously Administered Pozelimab in Combination with Cemdisiran or Cemdisiran Alone in Adult Participants with Geographic Atrophy. Identifier: NCT06541704. National Library of Medicine; 2024.
59. Burton MJ, Ramke J, Marques AP, Bourne RRA, Congdon N, Jones I, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Global Health. 2021;9(4):e489-e551.
60. Livingston G, Huntley J, Liu KY, Costafreda SG, Selbæk G, Alladi S, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024;404(10452):572-628.
61. GBD 2021 Global AMD Collaborators. Global burden of vision impairment due to age-related macular degeneration, 1990-2021, with forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Glob Health. 2025;13(7):e1175-e1190. doi:10.1016/S2214-109X(25)00143-3.
62. Tessier AJ, Wang F, Ardisson Korat A, Eliassen AH, Chavarro J, Grodstein F, et al. Optimal dietary patterns for healthy aging. Nature Medicine. 2025;31:1644-1652.
63. Swenor BK, Ehrlich JR. Ageing and vision loss: looking to the future. Lancet Glob Health. 2021;9(4):e385-e386. doi:10.1016/S2214-109X(21)00031-0.
64. Patel PJ, Ziemssen F, Ng E, et al. Burden of illness in geographic atrophy: a study of vision-related quality of life and health care resource use. Clin Ophthalmol. 2020;14:15-28. doi:10.2147/OPTH.S226425.
65. Colijn JM, Buitendijk GHS, Prokofyeva E, et al. Prevalence of age-related macular degeneration in Europe: the past and the future. Ophthalmology. 2017;124(12):1753-1763. doi:10.1016/j.ophtha.2017.05.035.
66. Fleckenstein M, Mitchell P, Freund KB, Sadda S, Holz FG, Brittain C, Henry EC, Ferrara D. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmology. 2018;125(3):369-390. doi:10.1016/j.ophtha.2017.08.038.
67. European Medicines Agency. Izelvay: withdrawal of application for marketing authorisation. Amsterdam: EMA; 2024.
68. Therapeutic Goods Administration. SYFOVRE (Apellis Australia Pty Ltd): prescription medicines registration. Canberra: TGA; 2025.
69. Therapeutic Goods Administration. IZERVAY (Astellas Pharma Australia Pty Ltd): prescription medicines registration; ARTG ID 447210. Canberra: TGA; 2025.
70. Astellas Pharma Inc. Astellas receives conditional approval for IZERVAY, making it the first and only approved treatment for the suppression of geographic atrophy growth in Japan. Tokyo: Astellas; 2025.
71. Astellas Pharma Inc. China’s National Medical Products Administration accepts New Drug Application for IZERVAY (avacincaptad pegol) for the treatment of geographic atrophy secondary to age-related macular degeneration. Tokyo: Astellas; 2026.
72. World Health Organization. Republic of Korea: WHO Listed Authority listing summary for the Ministry of Food and Drug Safety (MFDS). Geneva: WHO; 2025.
73. African Medicines Agency. Overview: African Medicines Agency. Kigali: AMA; 2025.
74. World Health Organization. WHO and African Medicines Agency launch landmark framework to strengthen access to quality-assured health products in Africa. Geneva: WHO; 2026.
75. Pan American Health Organization. Quality assurance of health technologies: national regulatory authorities of regional reference in the Americas. Washington, DC: PAHO; accessed 2026.
List of Figures
Summary list of infographic figures included in this flagship publication.
| Figure | Infographic image / title |
| Opening visual | Executive visual abstract – Age-related macular degeneration in an ageing world |
| Figure 1 | The Ageing Vision System |
| Figure 2 | The Sustainable Vision Care Framework |
| Figure 3 | The Longevity–Vision Paradox |
| Figure 4 | The Human Impact of AMD |
| Figure 5 | The Geographic Atrophy Transition Era |
| Figure 6 | A New Standard of Care |
| Figure 7 | The Home Care Advantage |
| Figure 8 | The Vision Ecosystem |
| Figure 9 | The Sustainable Vision Strategy |
| Figure 10 | The Lifetime Vision Journey |
