A Flagship Reference Publication on Preventable Blindness, Vision-System Resilience, and the Future of Vision Care
Dr. Samer Al-Diri
Author ORCID iD: 0009-0004-1908-0714 | https://orcid.org/0009-0004-1908-0714
Ophthalmology & Retina | Healthcare Management & Transformation | Healthcare AI | Public Health
Website | LinkedIn | X: @AldiriSamer
Positioning Statement
This flagship reference publication uses diabetic retinopathy as a model condition through which to examine the broader challenge of preventing avoidable blindness, strengthening vision-care systems, and advancing equitable, patient-centred, and technology-enabled eye care worldwide.
Although this publication focuses on diabetic retinopathy, the principles explored throughout—including prevention, screening, workforce development, responsible artificial intelligence, health-system resilience, and equitable access—apply broadly to the future of blindness prevention and vision care.
Related flagship publication: For a broader discussion of ageing, retinal disease burden, artificial intelligence, health-system capacity, and sustainable vision-care planning, see my flagship article on age-related macular degeneration, population ageing, health-system impact, artificial intelligence, and the future of sustainable vision care.
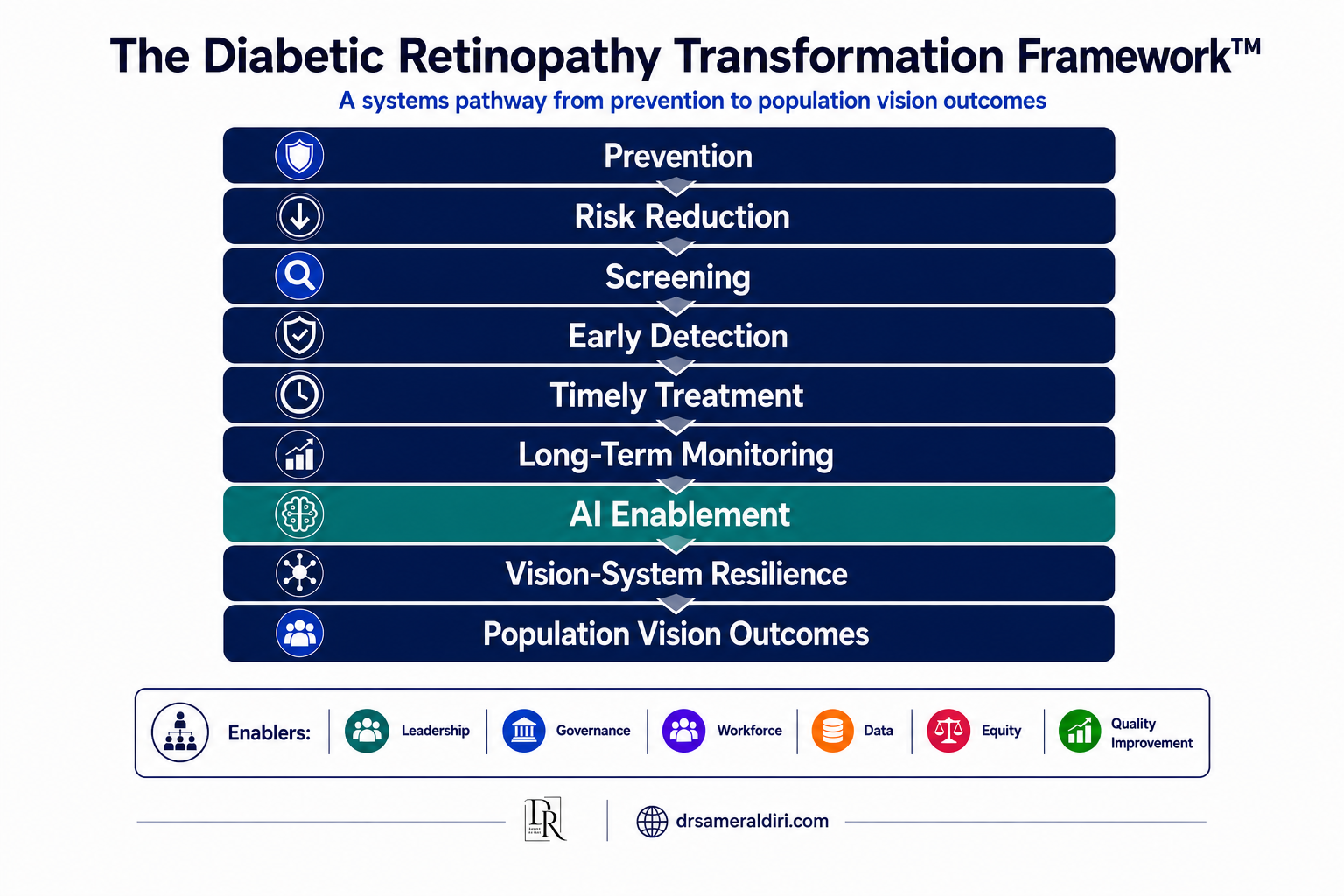
Figure 1. The Diabetic Retinopathy Transformation Framework™
A systems-based model illustrating how prevention, screening, treatment, monitoring, artificial intelligence, and health-system resilience interact to influence population vision outcomes. The framework emphasises that sustainable blindness prevention depends on the performance of the entire vision-care pathway rather than any individual intervention.
1. Executive Summary & Key Messages
Diabetic retinopathy remains one of the leading causes of preventable vision loss and blindness worldwide. Despite major advances in diabetes care, retinal imaging, organised screening programmes, pharmacological therapies, and artificial intelligence, avoidable vision loss continues to affect millions of people globally. [1–4]
This publication argues that diabetic retinopathy should be viewed not only as a retinal disease, but also as a public health challenge, a healthcare transformation challenge, and a health-system performance challenge. [1,5,27,29]
The central paradox is straightforward: effective preventive measures, screening strategies, and treatments already exist, yet many individuals continue to present with advanced disease that could have been detected and managed earlier. [3,6–9]
The future of diabetic retinopathy care will depend less on individual technological breakthroughs and more on the ability of healthcare systems to integrate prevention, screening, treatment, data, workforce development, and responsible innovation into coherent and resilient care pathways. [10,11,16,24,30]
Key Messages
- Much diabetic retinopathy-related blindness remains preventable.
- Prevention and screening are generally more effective than managing advanced disease.
- Health-system performance influences outcomes as much as clinical capability.
- Artificial intelligence should augment rather than replace clinical care.
- Equity must be embedded within vision-care systems rather than added later.
- Workforce development remains fundamental to sustainable blindness prevention.
- The future of vision care will be preventive, integrated, data-informed, and patient-centred.
Flagship Insight: The greatest challenge in diabetic retinopathy is no longer discovering how to treat disease—it is ensuring that effective prevention, screening, and treatment reach populations consistently, equitably, and sustainably.
2. The Diabetic Retinopathy Transformation Framework™
The Diabetic Retinopathy Transformation Framework™ provides the conceptual foundation for this publication. It proposes that outcomes are determined not by any single intervention, but by the performance of the entire vision-care pathway. Improvements in one stage cannot fully compensate for weaknesses elsewhere. Effective blindness prevention therefore requires coordinated action across multiple levels of the healthcare system.
The framework reinforces a simple but powerful principle: blindness prevention is a systems outcome. Healthcare systems with excellent treatments but poor screening will continue to experience avoidable blindness. Similarly, advanced AI tools cannot compensate for fragmented referral pathways, insufficient workforce capacity, weak governance, or poor patient engagement.
Figure 1. The Diabetic Retinopathy Transformation Framework™
A systems-based model illustrating how prevention, screening, treatment, monitoring, artificial intelligence, and health-system resilience interact to influence population vision outcomes. The framework emphasises that sustainable blindness prevention depends on the performance of the entire vision-care pathway rather than any individual intervention.
Flagship Insight: Sustainable blindness prevention depends on the performance of the entire vision-care pathway rather than any individual technology, treatment, or programme.
3. Key Terminology Registry
| Term | Definition |
| DR | Diabetic Retinopathy |
| DME | Diabetic Macular Edema |
| NPDR | Non-Proliferative Diabetic Retinopathy |
| PDR | Proliferative Diabetic Retinopathy |
| OCT | Optical Coherence Tomography |
| AI | Artificial Intelligence |
| Teleretinal Screening | Remote retinal assessment using digital imaging |
| Vision-System Resilience | The capacity of a health system to maintain vision-preserving functions while adapting to changing demands and external pressures |
| Preventable Blindness Paradox | The persistence of avoidable blindness despite effective prevention, screening, and treatment strategies |
| Programme Maturity | The degree to which a diabetic retinopathy programme has evolved from opportunistic detection to a coordinated, population-based system |
4. Introduction: The Preventable Blindness Paradox
Diabetic retinopathy occupies a unique position within modern healthcare. It is both a common complication of diabetes and one of the leading causes of preventable blindness among working-age adults. [1,4]
What makes diabetic retinopathy particularly important from a public health perspective is that much of the resulting vision loss can be prevented. Effective risk-factor management, organised screening programmes, timely referral, and evidence-based treatment strategies have repeatedly demonstrated their ability to reduce visual impairment. [3,6–9]
Yet despite these advances, diabetic retinopathy continues to cause substantial vision loss worldwide. This apparent contradiction forms the central narrative of this publication and may be described as the Preventable Blindness Paradox: avoidable blindness continues to occur despite the existence of effective prevention, screening, and treatment strategies.
Understanding this paradox requires moving beyond traditional clinical discussions and examining broader determinants of outcomes. Health-system performance, workforce capacity, accessibility, patient engagement, health literacy, equity, and policy decisions all influence whether evidence-based interventions reach the populations that need them. Accordingly, this publication approaches diabetic retinopathy not solely as a retinal disease but as a lens through which to examine the future of blindness prevention, healthcare transformation, and vision-system resilience.
Flagship Insight: The persistence of diabetic retinopathy-related blindness is not simply a clinical problem—it is a systems challenge extending across prevention, screening, treatment, policy, workforce, and equity.
5. Clinical Fundamentals
Diabetic retinopathy is a progressive microvascular complication of diabetes resulting from chronic hyperglycaemia and associated metabolic disturbances. Over time, retinal vascular damage may lead to increased vascular permeability, capillary closure, retinal ischemia, and pathological neovascularisation. These processes contribute to a spectrum of disease ranging from mild retinal abnormalities to advanced vision-threatening complications. [6,7,12,20,21]
Non-proliferative diabetic retinopathy (NPDR) represents the earlier stages of disease and is characterised by retinal microaneurysms, haemorrhages, exudates, venous abnormalities, and areas of retinal ischemia. Many individuals remain asymptomatic during these stages, highlighting the importance of regular retinal screening.
Proliferative diabetic retinopathy (PDR) develops when retinal ischemia stimulates the formation of abnormal new blood vessels. These vessels are fragile and may result in vitreous haemorrhage, tractional retinal detachment, and severe visual loss. [9,12]
Diabetic macular edema (DME) may occur at multiple stages of diabetic retinopathy and remains a major cause of vision impairment. Fluid accumulation within the macula can significantly affect central vision and quality of life. Risk is influenced by duration of diabetes, glycaemic control, blood pressure, lipid status, renal disease, and healthcare access. [8,12,21,23]
Importantly, diabetic retinopathy frequently progresses before symptoms develop.
Flagship Insight: The absence of symptoms does not indicate the absence of disease. By the time visual symptoms occur, opportunities for prevention may already have been lost.
6. Global Burden and Public Health Significance
The global prevalence of diabetes continues to increase, creating one of the most significant public health challenges of the twenty-first century. As the number of people living with diabetes grows, so too does the number at risk of developing diabetic retinopathy. [2,4,26]
The consequences extend beyond ophthalmology. Diabetic retinopathy affects workforce participation, healthcare expenditure, quality of life, social inclusion, and long-term health outcomes. It therefore represents not only an eye-health challenge but also a broader societal and economic concern. [1,5,27,29]
Significant variation exists between countries and regions. Some healthcare systems have established organised screening programmes and integrated referral pathways, while others continue to face limitations in workforce capacity, infrastructure, and access to specialist services. These disparities contribute to unequal outcomes despite the availability of effective interventions. [3–5,13,27,30]
From a public health perspective, diabetic retinopathy exemplifies the intersection of chronic disease management, prevention, health-system performance, and population health.
Flagship Insight: Diabetic retinopathy is not simply a retinal disease. It is a global public health challenge whose outcomes reflect the strengths and weaknesses of healthcare systems.
7. Human, Economic, and Caregiver Burden
The impact of diabetic retinopathy extends far beyond retinal pathology and visual acuity measurements. Vision loss influences independence, mobility, employment, education, social participation, mental well-being, and overall quality of life. [1,5,27,29]
For many individuals, visual impairment creates barriers to activities that are essential for daily living. Reading, driving, medication management, financial administration, and independent mobility may all become increasingly difficult. The consequences often extend beyond physical limitations and may contribute to social isolation, reduced confidence, anxiety, and loss of independence.
The economic burden is substantial. Direct costs include screening programmes, outpatient appointments, retinal imaging, pharmacological therapies, laser procedures, vitreoretinal surgery, rehabilitation services, and long-term care. Indirect costs may include reduced productivity, workforce absence, premature retirement, disability-related support, and loss of economic contribution. [5]
An often-overlooked dimension is the impact on caregivers. Family members frequently provide practical, emotional, and logistical support to individuals experiencing visual impairment. This contribution, while invaluable, may impose financial pressures, lost working time, emotional strain, and reduced quality of life for caregivers themselves.
The burden of diabetic retinopathy therefore extends beyond patients and healthcare providers. It affects families, communities, employers, healthcare systems, and national economies.
Flagship Insight: The true burden of diabetic retinopathy is measured not only in retinal damage or healthcare expenditure, but in lost independence, reduced opportunity, caregiver strain, and avoidable human suffering.
8. Health-System Impact and Workforce Pressure
The global growth of diabetes is creating substantial pressure on healthcare systems. As increasing numbers of individuals require retinal screening, monitoring, treatment, and long-term follow-up, demand is frequently outpacing available capacity. [2,4,26]
This challenge is particularly evident within ophthalmology and retina services, where workforce shortages, increasing referral volumes, and growing complexity of care may contribute to delays in assessment and treatment. However, diabetic retinopathy should not be viewed solely as an ophthalmology problem.
The condition exists at the intersection of primary care, diabetes services, endocrinology, public health, community healthcare, and specialist ophthalmology. Effective management therefore depends upon coordinated action across multiple sectors rather than the performance of any individual service. [10,11,30]
Workforce development represents one of the most important determinants of long-term success. Investment in training, leadership, service redesign, and multidisciplinary collaboration may ultimately yield greater benefits than isolated technological interventions.
Healthcare systems that fail to anticipate future demand risk widening the gap between service capacity and population needs.
Flagship Insight: The future challenge is not simply treating more patients—it is building sufficient workforce capacity and system capability to preserve vision at population scale.
9. The Diabetic Retinopathy Prevention Paradigm
The most effective strategy for reducing diabetic retinopathy-related blindness is not better treatment of advanced disease. It is preventing vision-threatening disease from developing in the first place.
This principle forms the foundation of the Diabetic Retinopathy Prevention Paradigm. Prevention begins long before retinal complications emerge. Effective diabetes management, glycaemic control, blood-pressure optimisation, lipid management, smoking cessation, patient education, and long-term engagement all contribute to reducing risk. [6,7,20,21]
Importantly, prevention should not be viewed as the responsibility of ophthalmology alone. Primary care clinicians, diabetes specialists, nurses, educators, public health professionals, policymakers, and patients themselves all play critical roles in maintaining retinal health.
Much blindness prevention occurs outside eye clinics. Primary care services often represent the first and most consistent point of contact for people living with diabetes. Opportunities to reinforce risk-factor control, encourage screening participation, identify barriers to care, and promote treatment adherence frequently arise within these settings. A prevention-focused system therefore requires strong integration between diabetes care and eye-care services. [10,11,30]
Flagship Insight: The most successful diabetic retinopathy programme is not the one that treats the most blindness—it is the one that prevents blindness from occurring.
10. Strengthening Screening Systems for the Modern Era
Screening remains one of the most effective interventions available for reducing diabetic retinopathy-related blindness. Because disease progression frequently occurs before symptoms develop, organised screening programmes create opportunities to identify individuals at risk before vision is threatened. [3,13,30]
However, screening should never be viewed as a standalone activity. Effective programmes depend upon a complete pathway encompassing invitation, attendance, image acquisition, interpretation, referral, treatment, and long-term follow-up. Weaknesses at any stage may reduce programme effectiveness and compromise outcomes.
Modern screening systems increasingly utilise digital imaging, teleretinal services, automated workflows, and integrated information systems. These innovations can improve accessibility, efficiency, and population coverage, particularly within underserved or geographically dispersed communities. [3,13,30]
Nevertheless, technology alone does not guarantee success. High-performing programmes are characterised by strong governance, quality assurance, workforce training, patient engagement, and continuous evaluation. [3,10]
Flagship Insight: Screening only creates value when it is connected to effective referral pathways, timely treatment, and sustained follow-up.
11. Emerging Treatments and Research Frontiers
Major advances in diabetic retinopathy management have transformed outcomes for many patients during the past two decades. Anti-vascular endothelial growth factor (anti-VEGF) therapies, corticosteroid-based treatments, laser interventions, and vitreoretinal surgery have significantly expanded the ability to preserve vision and manage complex disease. [8,9,22,23]
Future innovation is likely to focus on improving durability, personalisation, accessibility, and treatment efficiency. Key research priorities include longer-acting therapeutic agents, sustained drug-delivery systems, precision medicine approaches, biomarker-guided treatment strategies, gene- and cell-based therapies, and predictive analytics for disease progression.
Importantly, future success should not be measured solely by the introduction of new therapies. It should also be evaluated by the extent to which innovation improves accessibility, reduces treatment burden, and contributes to better population outcomes.
Flagship Insight: The future of diabetic retinopathy treatment is not simply stronger therapies—it is more accessible, durable, personalised, and sustainable care.
12. Cost-Effectiveness of Screening versus Treatment
Healthcare resources are finite, while the burden of diabetes and diabetic retinopathy continues to grow. This reality requires policymakers and healthcare leaders to consider not only clinical effectiveness but also economic sustainability. [4,5]
The evidence consistently supports investment in prevention, screening, and early intervention. Although organised screening programmes require infrastructure, workforce, technology, and quality assurance, these investments are often substantially less costly than managing advanced disease and its long-term consequences. [3,5]
The economic burden of visual impairment extends beyond healthcare expenditure. Productivity losses, disability-related costs, reduced workforce participation, and caregiver impacts may create substantial societal costs. Cost-effectiveness should therefore be viewed through a broad societal lens rather than a narrow healthcare accounting perspective.
Healthcare systems that detect disease earlier are more likely to preserve vision, reduce treatment burden, minimise complications, and improve long-term sustainability.
Flagship Insight: Blindness is substantially more expensive than prevention. The most cost-effective diabetic retinopathy strategy is often preventing vision-threatening disease rather than managing its consequences.
13. Artificial Intelligence in Diabetic Retinopathy
Artificial intelligence (AI) represents one of the most significant developments in diabetic retinopathy care. Advances in machine learning and retinal image analysis have demonstrated the potential to support screening, improve efficiency, expand access, and strengthen health-system capacity. [14,15,24,25]
The greatest opportunity for AI lies not in replacing clinicians but in addressing one of the most persistent challenges highlighted throughout this publication: the gap between the number of people requiring eye care and the capacity of health systems to provide it.
AI-assisted retinal image analysis can help identify individuals with referable diabetic retinopathy, prioritise high-risk patients, and support more efficient referral pathways. In settings facing workforce shortages or increasing demand, these capabilities may improve access to timely assessment while reducing pressure on specialist services. [15,25]
Beyond screening, AI may contribute to risk stratification, workflow optimisation, population health management, and clinical decision support. As data integration improves, future systems may help identify patients at increased risk of progression, enabling more proactive and personalised models of care.
However, technological capability alone does not guarantee better outcomes. Successful implementation requires rigorous validation, clinical oversight, governance frameworks, regulatory accountability, and ongoing quality assurance. Algorithms trained in one population may not perform equally well in another. Data quality, representativeness, and transparency remain critical considerations. [16,24,25]
Equity must also remain central. When implemented responsibly, AI can help extend screening capacity into underserved regions and support more equitable access to care.
Flagship Insight: The greatest value of artificial intelligence may not be replacing clinicians, but extending access to timely, equitable, and vision-preserving care through stronger and more efficient health systems.
14. Health Equity and Global Disparities
Diabetic retinopathy affects people in every region of the world, yet the risk of vision loss is not distributed equally. In many settings, outcomes are influenced not only by disease severity but also by where people live, their socioeconomic circumstances, and their ability to access timely care. [5,17,30]
Low- and middle-income countries often face challenges including workforce shortages, limited retinal imaging capacity, fragmented referral pathways, and restricted access to specialist services. These barriers may delay diagnosis and treatment, increasing the likelihood of avoidable vision loss.
However, inequities are not confined to resource-limited settings. Significant disparities also exist within high-income countries, where socioeconomic deprivation, rurality, transportation barriers, health literacy, and unequal access to healthcare services can influence screening uptake and treatment adherence.
Addressing diabetic retinopathy therefore requires more than clinical innovation alone. It requires deliberate efforts to improve accessibility, strengthen healthcare infrastructure, expand workforce capacity, and ensure that advances in screening, treatment, and artificial intelligence benefit all populations.
Flagship Insight: Where a person lives, their socioeconomic circumstances, and their access to healthcare can influence outcomes as much as disease itself. Equity must be designed into vision-care systems rather than added later.
15. Why Health Systems Continue to Struggle with Diabetic Retinopathy
Given the availability of effective preventive measures, organised screening programmes, advanced imaging technologies, proven treatments, and emerging artificial intelligence solutions, an important question remains: why does diabetic retinopathy continue to cause avoidable vision loss on such a large scale?
The answer lies not in a single failure, but in the cumulative effect of multiple weaknesses across the vision-care pathway. Several recurring patterns emerge across healthcare systems: fragmented care pathways, low screening participation, delayed referral and treatment, workforce shortages, limited data integration, reactive rather than preventive care, and unequal access to services. Viewed collectively, these challenges reveal a broader reality: diabetic retinopathy is not solely a retinal disease problem. It is also a systems-design challenge. [3,10,11,30]
The Diabetic Retinopathy Programme Maturity Model™
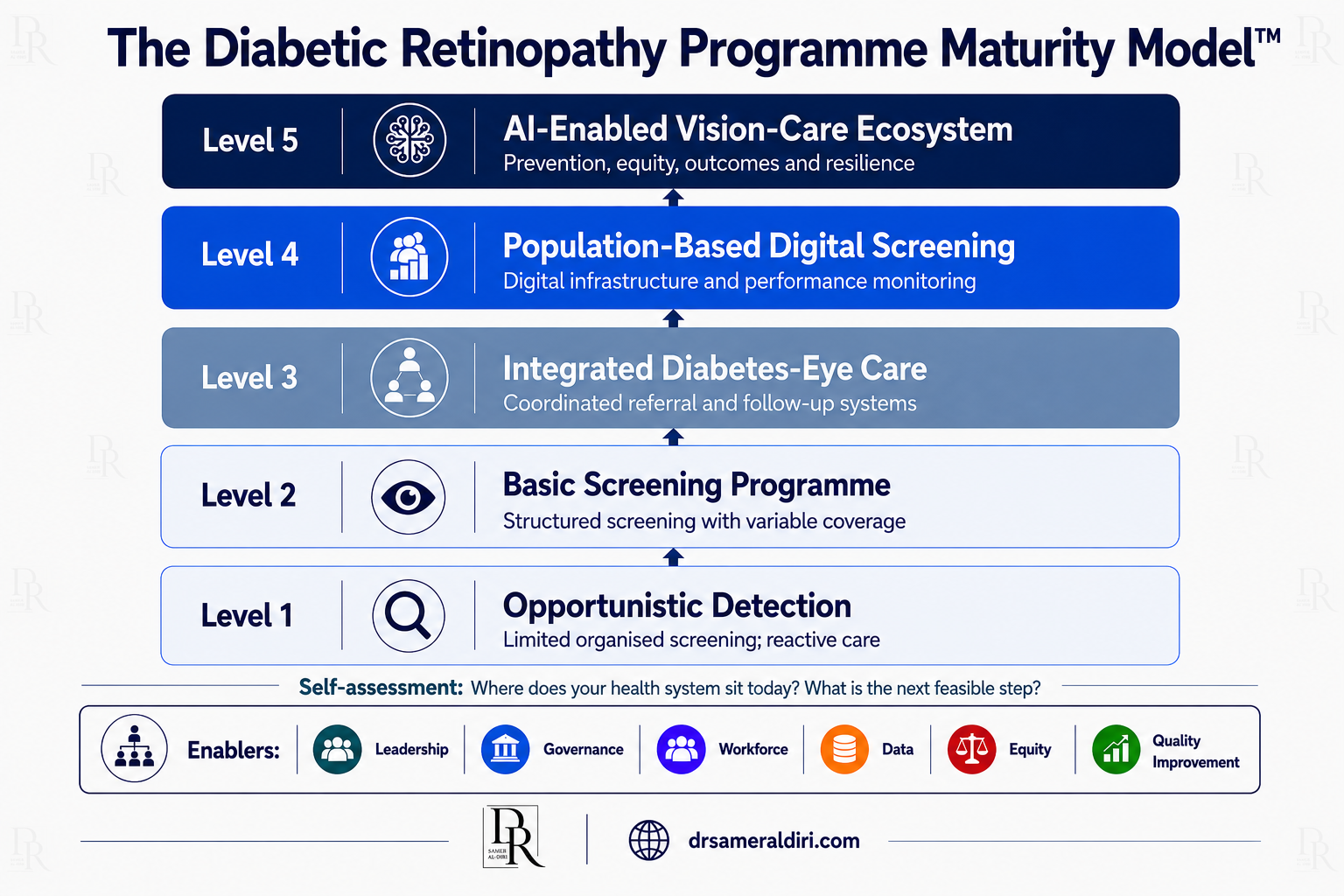
Figure 2. The Diabetic Retinopathy Programme Maturity Model™
A maturity model illustrating the five developmental stages of diabetic retinopathy programmes, from opportunistic detection to an AI-enabled, continuously improving vision-care ecosystem. The model emphasises that progression through maturity levels depends on strengthening prevention, screening, referral pathways, workforce capability, governance, data infrastructure, equity, quality improvement, and long-term vision-system resilience. The objective is not technological sophistication for its own sake, but strengthening the pathway from prevention to vision preservation.
Vision-System Resilience
Vision-System Resilience may be defined as: the capacity of a health system to maintain essential vision-preserving functions, absorb operational pressures and external shocks, adapt to changing population needs, and continue delivering effective care over time. [18,19]
While health-system resilience has become an increasingly important concept within global health, its application to eye care has received comparatively limited attention. Yet diabetic retinopathy demonstrates clearly why resilience matters.
Vision-care systems face multiple pressures simultaneously, including increasing diabetes prevalence, ageing populations, workforce shortages, rising demand for specialist services, technological disruption, financial constraints, and occasional large-scale shocks such as pandemics or humanitarian crises. A resilient vision-care system does more than respond to these pressures. It anticipates them.
At the clinical level, resilience involves maintaining access to screening, diagnosis, treatment, and follow-up services despite fluctuations in demand. At the organisational level, it requires workforce development, data-driven decision-making, service integration, and continuous quality improvement. At the national level, resilience depends upon sustainable financing, effective governance, strategic planning, and long-term commitment to blindness prevention.
Importantly, resilience is not synonymous with efficiency. Highly efficient systems may operate effectively under normal conditions yet struggle when demand increases unexpectedly. Resilient systems are designed not only for performance, but also for adaptation.
Viewed through this lens, Vision-System Resilience becomes a central objective of modern blindness prevention and a practical framework for linking clinical excellence, public health strategy, healthcare transformation, and responsible innovation.
Flagship Insight: The ultimate goal is not merely treating diabetic retinopathy more effectively. It is creating resilient vision-care systems capable of preserving sight consistently, equitably, and sustainably across entire populations.
16. Future of Vision Care: Integrated, Preventive, AI-Enabled Models
The future of diabetic retinopathy care will be defined not by a single breakthrough technology or therapy, but by the successful integration of prevention, screening, treatment, data, workforce capacity, and responsible innovation into a cohesive vision-care ecosystem. [10,11,16,24,30]
Historically, many healthcare systems have operated reactively, intervening after disease progression has already occurred. A more effective model is emerging: prevention is prioritised alongside treatment; screening is embedded within routine diabetes care; referral pathways are coordinated and efficient; data systems support continuity of care; artificial intelligence assists with capacity, triage, and risk stratification; and clinical teams focus increasingly on proactive intervention.
Technology does not replace human judgement. Instead, it enables healthcare professionals to work more effectively within integrated systems designed around patient needs and population outcomes.
Flagship Insight: The future of vision care will be preventive, integrated, data-informed, AI-enabled, and patient-centred. Success will depend not on individual innovations but on how effectively health systems combine them into resilient pathways that preserve sight at population scale.
17. Call to Action for the Next Decade & Executive Policy Brief
The global burden of diabetic retinopathy is expected to increase as diabetes prevalence continues to rise. Yet unlike many health challenges, much of the resulting vision loss is preventable. The knowledge exists. The screening technologies exist. The treatments exist. Increasingly, the digital tools and artificial intelligence capabilities exist. [1–5,14–16,24,25]
The central challenge is no longer whether avoidable blindness can be reduced. The challenge is whether health systems can act with sufficient urgency, coordination, and vision to translate these opportunities into population-level outcomes.
Executive Policy Brief
For Health Ministers
- Prioritise diabetic retinopathy within national diabetes and non-communicable disease strategies.
- Expand access to organised screening programmes.
- Strengthen data systems and programme evaluation.
For Healthcare Leaders and Hospital CEOs
- Strengthen referral pathways and service integration.
- Invest in workforce development and long-term capacity building.
- Embed prevention within organisational strategy.
For Public Health Agencies
- Improve screening participation and community awareness.
- Address barriers affecting underserved populations.
- Promote equitable access to vision-preserving services.
For Ophthalmology and Retina Leaders
- Champion prevention alongside treatment.
- Support integrated models of care and responsible AI adoption.
- Strengthen collaboration across the diabetes care pathway.
The next decade offers a once-in-a-generation opportunity to move from reactive treatment toward proactive prevention, integrated screening, responsible artificial intelligence, and resilient vision-care systems capable of preserving sight at population scale.
Flagship Insight: The question is no longer whether avoidable blindness can be reduced. The question is whether health systems are prepared to act with sufficient urgency, coordination, and vision to make it happen.
Methodology
This flagship reference publication was developed through a narrative synthesis of evidence drawn from major international organisations, peer-reviewed medical journals, public-health literature, health-systems research, and artificial-intelligence governance frameworks.
Sources were selected based on scientific credibility, international authority, clinical relevance, policy significance, and contribution to understanding diabetic retinopathy as a clinical, public-health, healthcare transformation, and health-system challenge.
Particular emphasis was placed on evidence and guidance from leading institutions and publications including the World Health Organization (WHO), International Diabetes Federation (IDF), The Lancet, Lancet Global Health, The New England Journal of Medicine (NEJM), Nature Medicine, Ophthalmology, JAMA Ophthalmology, Moorfields Eye Hospital, Harvard Medical School, Johns Hopkins University, and the London School of Hygiene & Tropical Medicine (LSHTM).
The publication intentionally emphasises enduring principles—including prevention, screening, health-system resilience, workforce development, responsible artificial intelligence, and equitable access—rather than focusing solely on specific technologies or therapies that may evolve over time.
Final Reflection
Diabetic retinopathy illustrates both the achievements and limitations of modern healthcare.
The knowledge required to prevent much avoidable blindness already exists. Effective prevention strategies, organised screening programmes, evidence-based treatments, and increasingly sophisticated digital technologies have transformed what is possible.
Yet knowledge alone does not preserve sight.
The challenge for the coming decade is not discovering what works, but ensuring that prevention, screening, treatment, innovation, and equity are translated into sustainable population outcomes.
Ultimately, the future of vision care will be determined not by technology alone, but by the collective ability of health systems to preserve sight before it is lost.
If diabetic retinopathy teaches one lesson above all others, it is this: preventable blindness should no longer be accepted as an inevitable consequence of disease when the tools to prevent it already exist.
About the Author
Dr. Samer Al-Diri
Ophthalmology & Retina | Healthcare Management & Transformation | Healthcare AI | Public Health
Dr. Samer Al-Diri is an ophthalmologist with a multidisciplinary background spanning ophthalmology and retina, healthcare management, healthcare transformation, healthcare AI, public health, global health, leadership, governance, and health-systems strengthening. His work focuses on patient-centred care, sustainable healthcare transformation, responsible AI adoption, health equity, and the future of healthcare delivery.
Website: https://drsameraldiri.com
LinkedIn: https://www.linkedin.com/in/dr-samer-al-diri
Keywords
Diabetic Retinopathy; Preventable Blindness; Vision-System Resilience; Healthcare AI; Public Health; Retina; Health Systems Strengthening; Artificial Intelligence in Ophthalmology; Diabetic Retinopathy Screening; Global Eye Health; Healthcare Transformation; Future of Vision Care
References and Source Links
1. World Health Organization. World report on vision. Geneva: World Health Organization; 2019.
2. International Diabetes Federation. IDF Diabetes Atlas. 11th ed. Brussels: International Diabetes Federation; 2025.
3. World Health Organization Regional Office for Europe. Diabetic retinopathy screening: a short guide. Copenhagen: WHO Regional Office for Europe; 2020.
4. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027.
5. Burton MJ, Ramke J, Marques AP, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5.
6. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–986. doi:10.1056/NEJM199309303291401.
7. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes. BMJ. 1998;317(7160):703-713. DOI: 10.1136/bmj.317.7160.703
8. Wells JA, Glassman AR, Ayala AR, et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-1203. DOI: 10.1056/NEJMoa1414264
9. Gross JG, Glassman AR, Jampol LM, et al. Panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2015;314(20):2137-2146. DOI: 10.1001/jama.2015.15217
10. World Health Organization. Package of eye care interventions. Geneva: World Health Organization; 2022.
11. World Health Organization. Integrated people-centred eye care, including preventable vision impairment and blindness. Geneva: World Health Organization; 2020.
12. Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic colour fundus photographs: an extension of the modified Airlie House classification. Ophthalmology. 1991;98(5 Suppl):786–806.
13. NHS England. Diabetic eye screening programme overview. GOV.UK.
14. De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24(9):1342-1350. DOI: 10.1038/s41591-018-0107-6
15. Abràmoff MD, Lavin PT, Birch M, et al. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digit Med. 2018;1:39. DOI: 10.1038/s41746-018-0040-6
17.Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: World Health Organization; 2008.
18. Kruk ME, Myers M, Varpilah ST, Dahn BT. What is a resilient health system? Lessons from Ebola. Lancet. 2015;385(9980):1910-1912. DOI: 10.1016/S0140-6736(15)60755-3
19. Kruk ME, Ling EJ, Bitton A, et al. Building resilient health systems: a proposal for a resilience index. BMJ. 2017;357:j2323. DOI: 10.1136/bmj.j2323
20. American Diabetes Association Professional Practice Committee. 12. Retinopathy, neuropathy, and foot care: Standards of Care in Diabetes-2026. Diabetes Care. 2026;49(Suppl 1):S261-S276. DOI: 10.2337/dc26-S012
22. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741–755. DOI: 10.1016/S0140-6736(22)00018-6.
23. Jhaveri CD, Glassman AR, Ferris FL 3rd, et al. Aflibercept monotherapy or bevacizumab first for diabetic macular edema. N Engl J Med. 2022;387(8):692-703. DOI: 10.1056/NEJMoa2204225
24. Tan TF, Thirunavukarasu AJ, Jin L, et al. Artificial intelligence and digital health in global eye health: opportunities and challenges. Lancet Glob Health. 2023;11(9):e1432-e1443. DOI: 10.1016/S2214-109X(23)00323-6
25. US Food and Drug Administration. FDA permits marketing of artificial intelligence-based device to detect diabetic retinopathy in primary care. Silver Spring, MD: US Food and Drug Administration; 2018.
26. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556-564. DOI: 10.2337/dc11-1909
27. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221-e1234. DOI: 10.1016/S2214-109X(17)30393-5
28. World Health Organization. International classification of functioning, disability and health: ICF. Geneva: World Health Organization; 2001.
29. Brown MM, Brown GC, Sharma S, Shah G. Utility values and diabetic retinopathy. Am J Ophthalmol. 1999;128(3):324-330. doi: 10.1016/S0002-9394(99)00146-4
30. World Health Organization. Eye care in health systems: guide for action. Geneva: World Health Organization; 2022.

